# Learning objectives
Types and Flow Profiles of Prosthetic Valves
人工瓣膜的类型和血流动力学特征Echocardiographic Evaluation: Key Points
超声评估要点Prosthetic Valves Evaluation:
- Elevated gradients 跨瓣压差
- Regurgitation 反流
- Endocarditis 心内膜炎
- Thrombus versus Pannus 血栓与血管翳的鉴别
Challenges for Evaluation 困难和挑战
# Basic Echo Evaluation
Clinical Information 临床信息
- Date of valve replacement 换瓣时间
- Type and Size of the prosthetic valve 人工瓣膜类型和大小
- Height/Weight/Body surface area 身高 / 体重 / 身体表面积
- Symptoms and clinical findings 症状和临床发现
- Blood pressure and heart rate 血压和心率
Imaging of the valve 瓣膜的成像
- Motion of leaflets /occluder 瓣叶 / 假体的运动
- Presence of calcification on the leaflets or abnormal echo density on various components of the prosthesis
瓣叶上有钙化或假体各部分有异常回声密度 - Valve sewing ring integrity and motion
瓣膜缝纫环的完整性和运动
# Types and Flow Profiles - Mechanical vs. Bioprosthetic vs. Autografts 类型和流动剖面 - 机械瓣 vs. 生物瓣 vs. 自体移植物
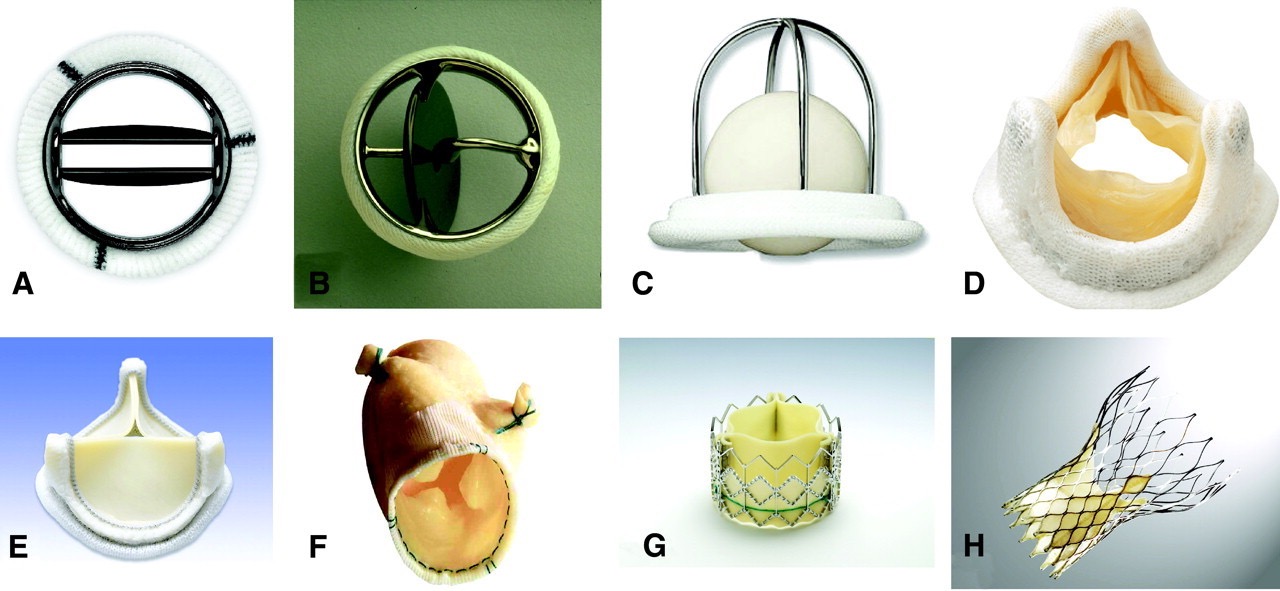
- Different types of prosthetic valves. [1]
- Mechanical 机械瓣
- A, Bileaflet mechanical valve (St Jude); 双叶瓣
- B, monoleaflet mechanical valve (Medtronic Hall); 单叶瓣
- C, caged ball valve (Starr-Edwards); 球笼瓣
- Biologic 生物瓣
- Stented 有支架的
- D, stented porcine bioprosthesis (Medtronic Mosaic); 猪心瓣
- E, stented pericardial bioprosthesis (Carpentier-Edwards Magna); 心包
- Stentless 无支架的
- F, stentless porcine bioprosthesis (Medtronic Freestyle);
- Percutaneous 经皮
- G, percutaneous bioprosthesis expanded over a balloon (Edwards Sapien); 球扩瓣
- H, self-expandable percutaneous bioprosthesis (CoreValve). 自膨瓣
- Stented 有支架的
# Bioprosthetic Valve Dysfunction 生物瓣膜功能障碍
- Structural Valve Deterioration 瓣膜结构性衰败
- Intrinsic permanent changes of the prosthetic valve (i.e., calcification, leaflet fibrosis, tear or flail) leading to degeneration and/or dysfunction
人工瓣膜的内在永久性变化(即钙化、瓣叶纤维化、撕裂或连枷)导致退化和 / 或功能障碍 - Nonstructural Valve Deterioration 非结构性衰败
- Any abnormality not intrinsic to the prosthetic valve itself (i.e., intra- or para-prosthetic regurgitation, prosthesis malposition, patient-prosthesis mismatch, late embolization) leading to degeneration and/or dysfunction
任何与人工瓣膜本身无关的异常(即瓣中或瓣周反流、假体错位、患者 - 人工瓣膜不匹配、晚期栓塞)导致退化和 / 或功能障碍 - Thrombosis 血栓形成
- Thrombus development on any structure of the prosthetic valve, leading to dysfunction with or without thrombo-embolism
人工瓣膜任何结构上的血栓形成,导致功能障碍伴或不伴血栓栓塞 - Endocarditis 心内膜炎
- Infection involving any structure of the prosthetic valve, leading to perivalvular abscess, dehiscence, pseudo-aneurysms, fistulae, vegetations, cusp rupture or perforation
感染涉及人工瓣膜的任何结构,导致瓣膜周围脓肿、裂开、假性动脉瘤、瘘管、赘生物、瓣尖破裂或穿孔
# Mechanism of Prosthetic Valve Dysfunction 人工瓣膜功能障碍的机制

# Classification 分类
# of Mechanical Valves 机械瓣
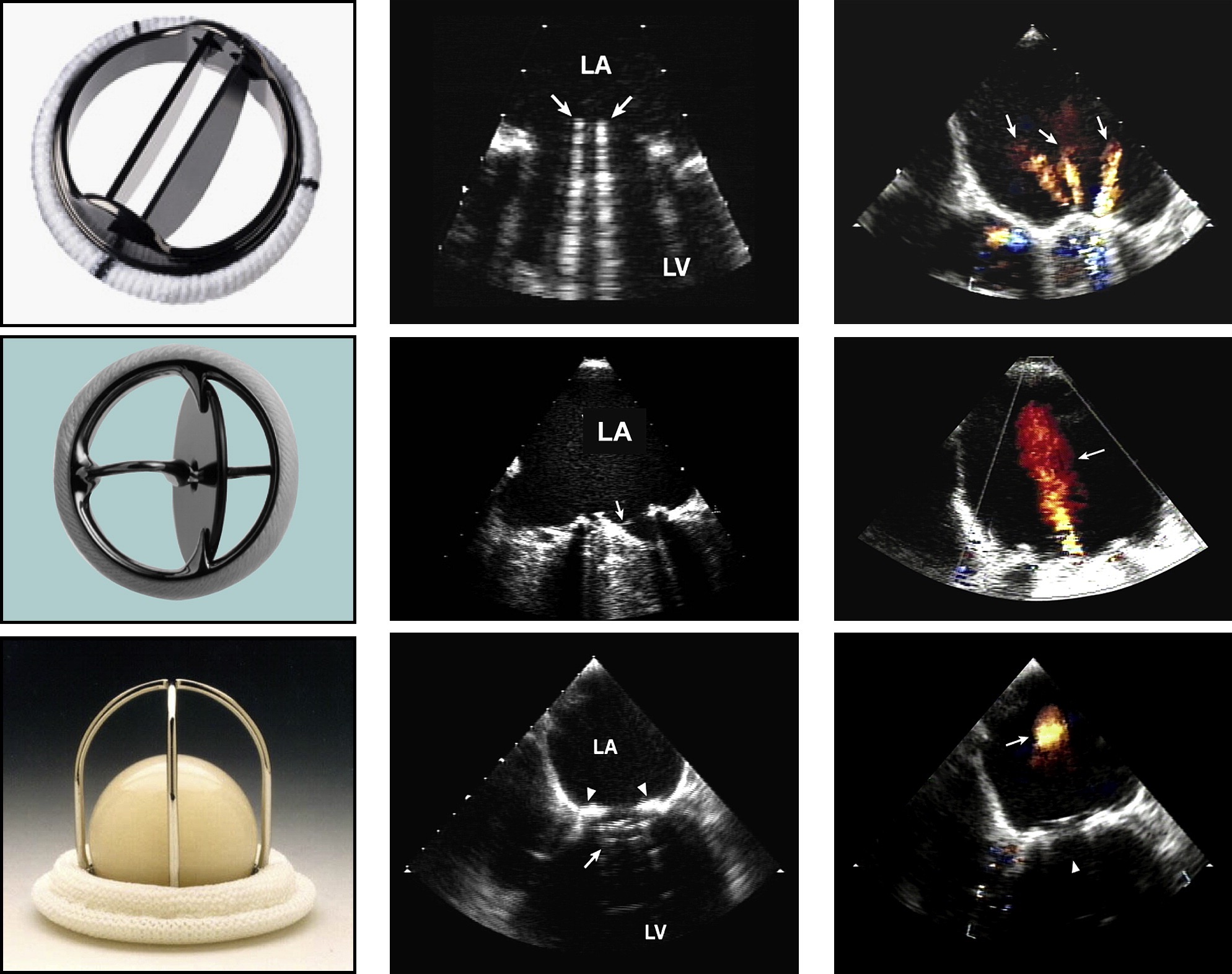
Examples of (A) bileaflet, (B) single-leaflet, and (C) caged-ball mechanical valves and their transesophageal echocardiographic characteristics taken in the mitral position in diastole (middle) and in systole (right). [2]
(A) 双叶瓣、(B) 单叶瓣和 (C) 笼形球状机械瓣及其在二尖瓣位置舒张期 (中) 和收缩期 (右) 的经食道超声心动图特征。
The arrows in diastole point to the occluder mechanism of the valve and in systole to the characteristic physiologic regurgitation observed with each valve.
舒张期的箭头指向瓣膜的封堵机制,而收缩期的箭头指向观察到的每个瓣膜特有的生理性反流。
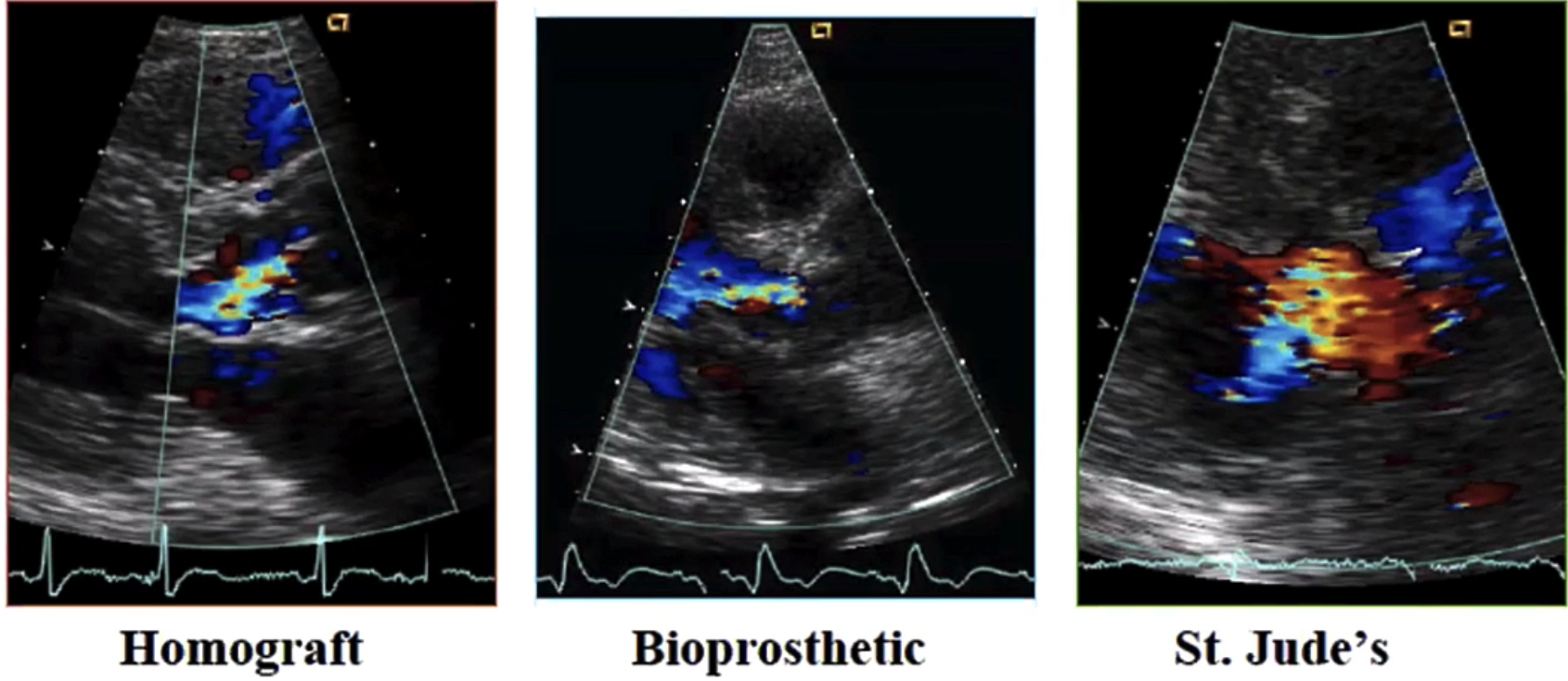
# of Biologic Valves 生物瓣
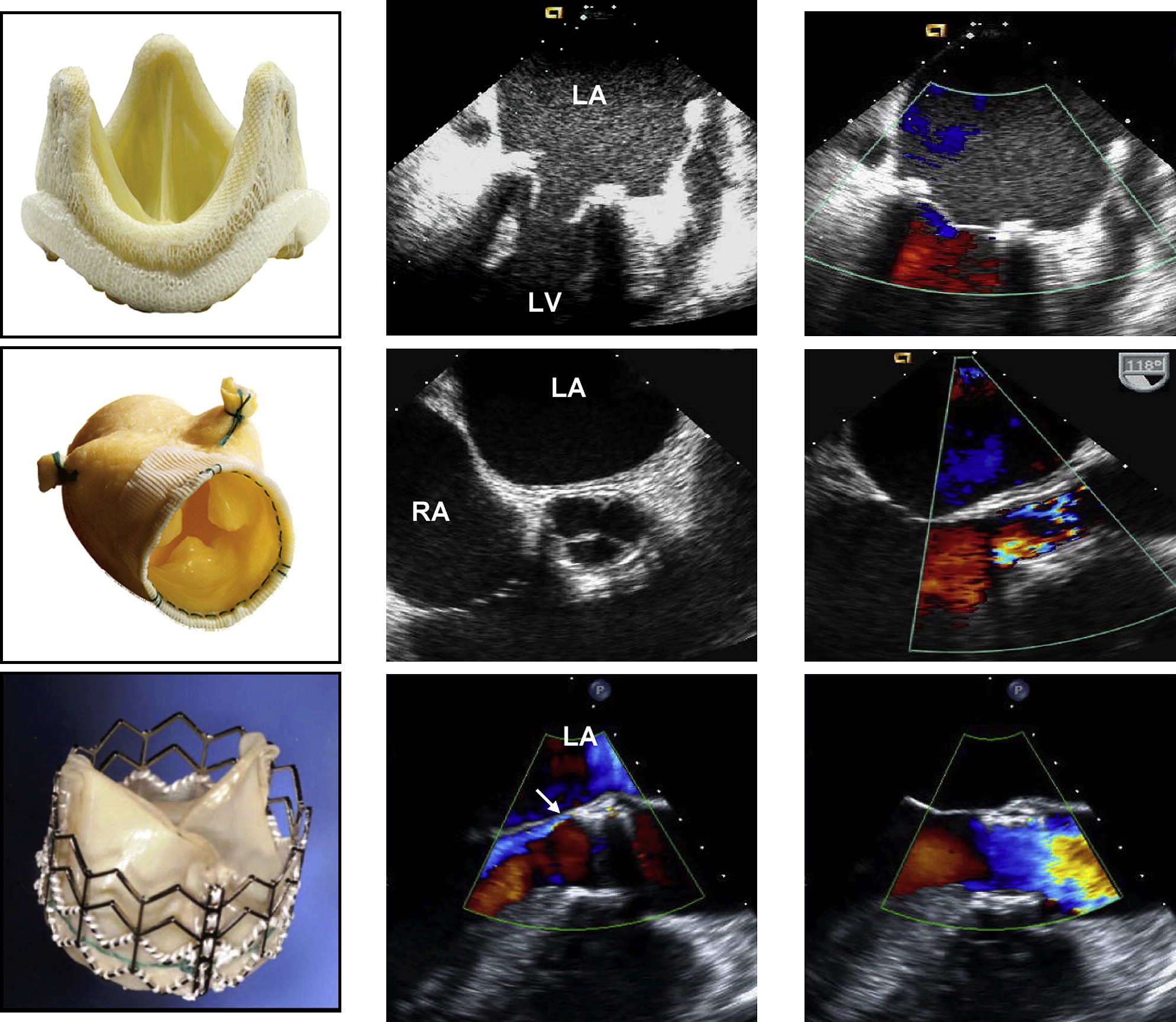
Examples of (A) stented, (B) stentless, and (C) percutaneous biologic valves and their echocardiographic features in diastole (middle) and in systole (right) as seen by transesophageal echocardiography. [2]
经食道超声心动图显示 (A) 有支架、(B) 无支架和 (C) 经皮生物瓣膜及其舒张期 (中) 和收缩期 (右) 的超声心动图特征。
The stentless valve is inserted by the root inclusion technique.
无支架瓣膜是通过根部包裹技术植入的。
Mild perivalvular aortic regurgitation in the percutaneous valve is shown by the arrow.
箭头所示为经皮瓣膜轻度主动脉瓣周反流。
# Doppler Echo Evaluation of AVR 主动脉瓣人工瓣膜
- Contour of the jet velocity signal 射流速度信号的轮廓
- Peak velocity and gradient 峰值速度和压差
- Mean pressure gradient 平均跨瓣压差
- Velocity-time integral of the jet 射流的速度 - 时间积分
- Presence, location and severity of regurgitation 反流的存在、位置和严重程度
- Effective orifice area 有效瓣口面积
# Doppler Parameters of Prosthetic Aortic Valve Function in Mechanical and Stented Biological Valves 机械瓣膜和带支架生物瓣膜人工主动脉瓣功能的多普勒参数
In conditions of normal or near normal stroke volume prough the aortic valve.
在每搏量正常或接近正常的情况下,通过主动脉瓣的血流进行多普勒超声检查
Normal | Possible Stenosis | Suggests Significant Stenosis | |
|---|---|---|---|
Peak velocity | < 3 m/s | 3-4 m/s | > 4 m/s |
Mean gradienty | < 20 mmHg | 20-35 mmHg | > 35 mmHg |
Doppler velocity index | ≥ 0.30 | 0.29-0.25 | < 0.25 |
Effective orifice area | > 1.2cm2 | 1.2-0.8 cm2 | < 0.8 cm2 |
Contour of the jet velocity through the PrAV | Triangular, Early peaking | Triangular to Intermediate | Rounded, symmetrical contour |
Acceleration time | < 80ms | 80-100 ms | > 100 ms |
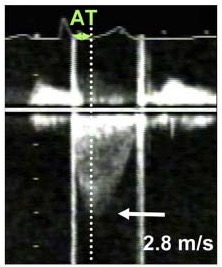
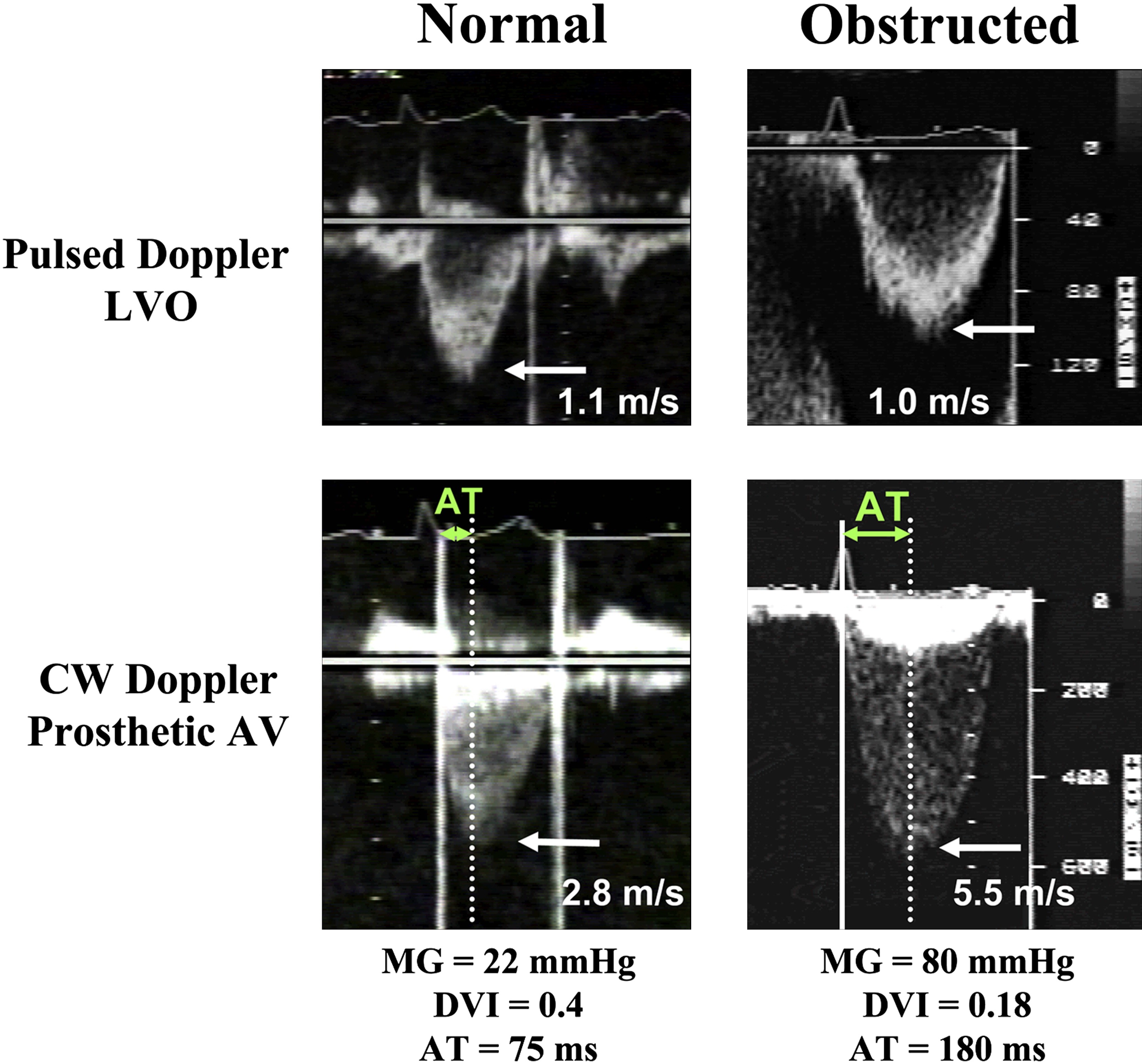
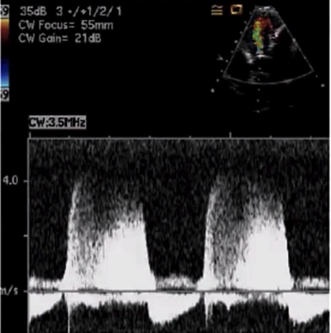
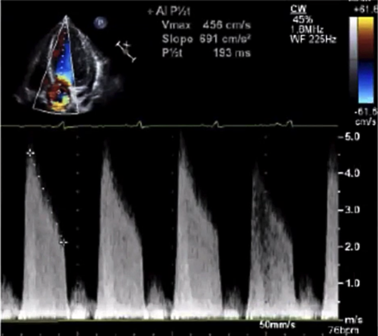
# Jet Contour (Prosthetic Aortic valve) 射流束频谱轮廓(人工主动脉瓣)


# Peak Velocity (Prosthetic Aortic valve) 峰值速度
| Normal | Abnormal | |
|---|---|---|
CW Doppler Prosthetic AV |
|
|
| AT 加速时间 | < 100 msec | > 100 msec |

# Doppler Velocity Index (DVI) 多普勒速度比
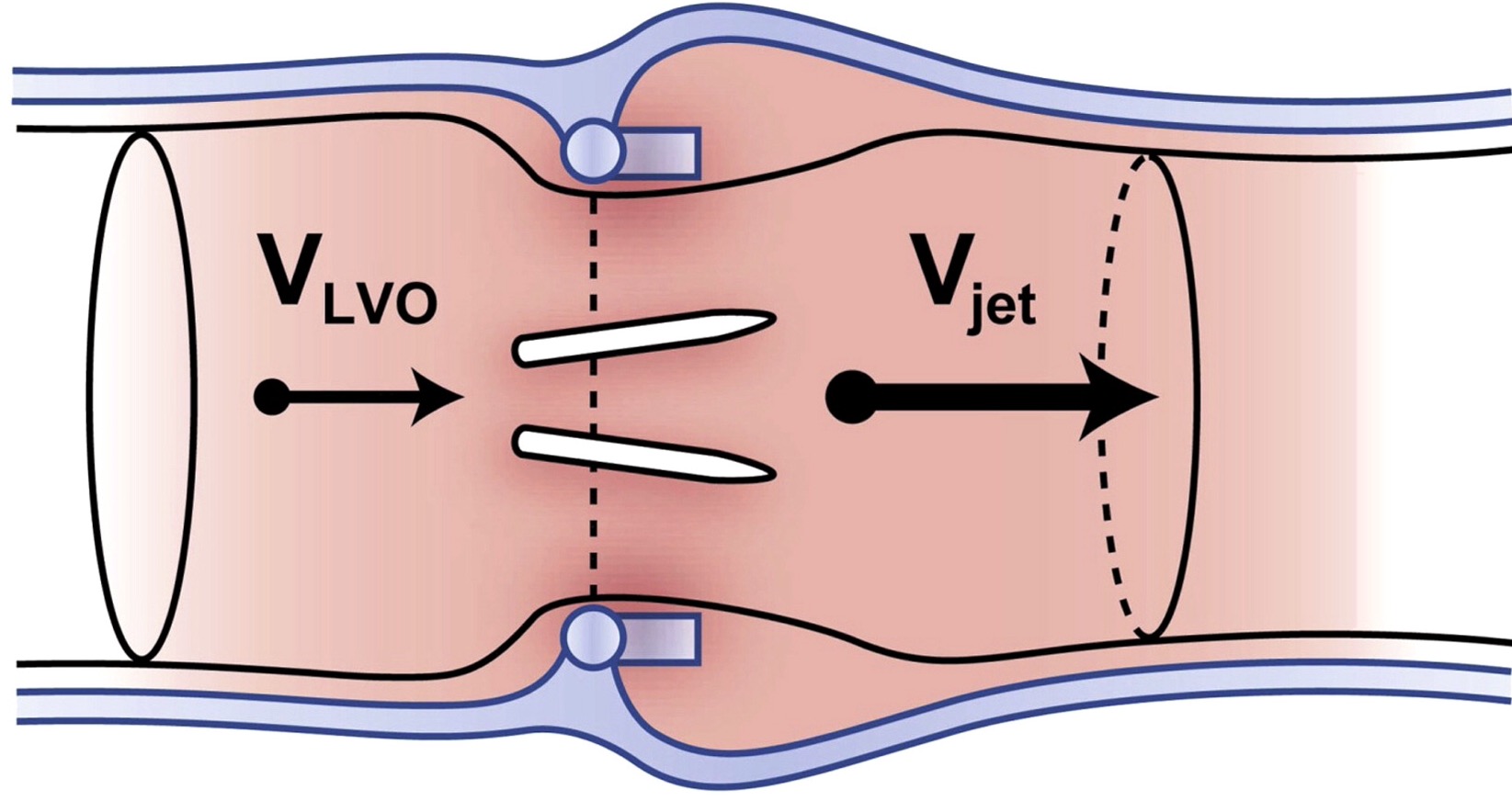
- 在左室流出道进行 PW 的测量 (Pulsed Doppler LVO)
- CW 测经瓣口的血流最大峰值 (CW Doppler Prosthetic AV)
| Normal | Obstructed |
|---|---|
| > 0.3 | < 0.25 |
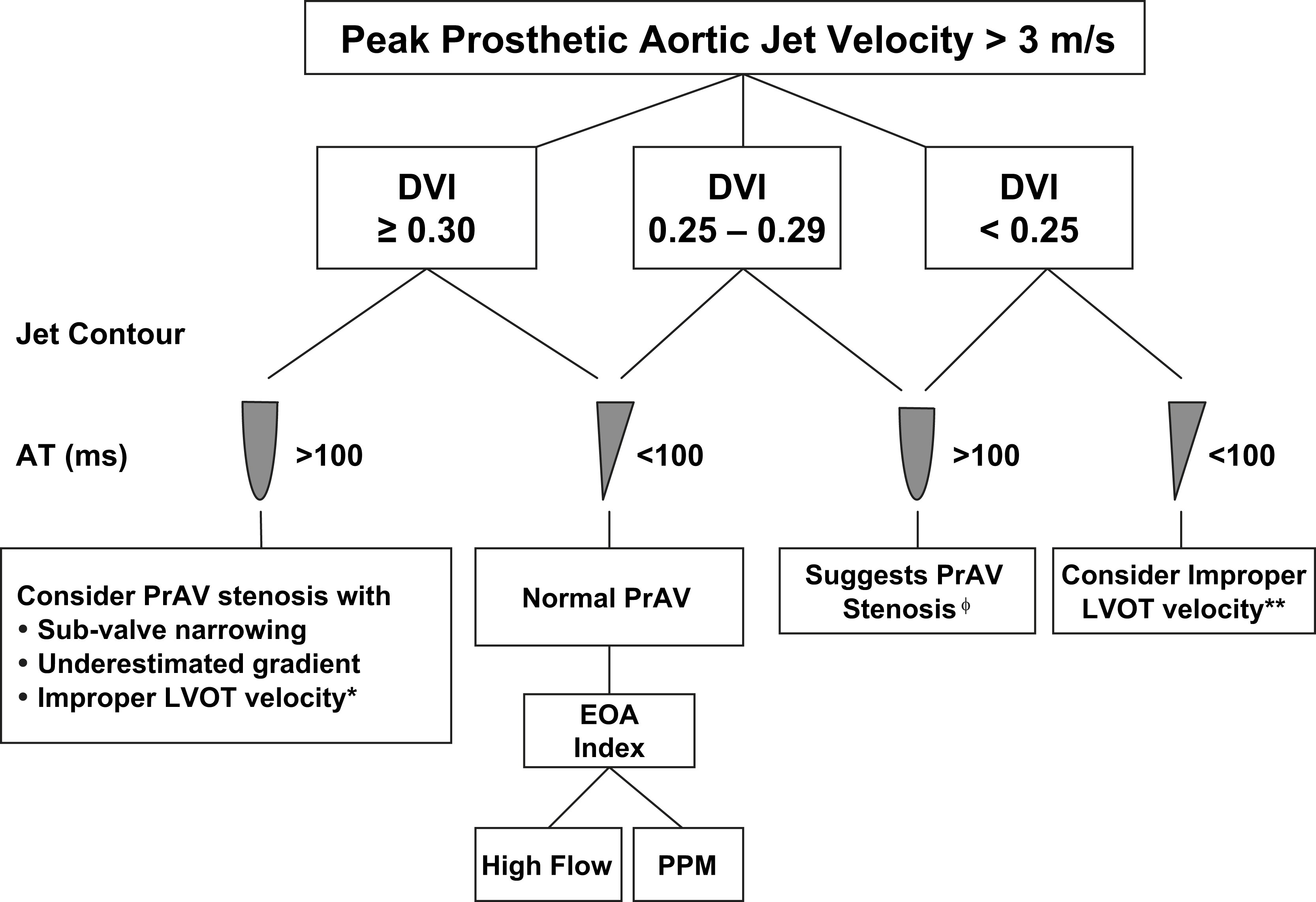
- 通过射流速度,先算 DVI
- 然后根据频谱形态轮廓和加速时间再细分
- 区分是正常的人工瓣膜,还是提示狭窄
Consider PrAV stenosis with 考虑人工瓣膜狭窄并且
- Sub-valve narrowing 瓣下狭窄
- Underestimated gradient 低估的跨瓣压差
- Improper LVOT velocity LVOT 速度测量不当
正常的人工瓣膜
Suggests PrAV Stenosis 提示人工瓣膜狭窄
三个指标都相符Consider Improper LVOT velocity LVOT 速度测量不当
# Effective Orifice Area (EOA) 有效瓣口面积
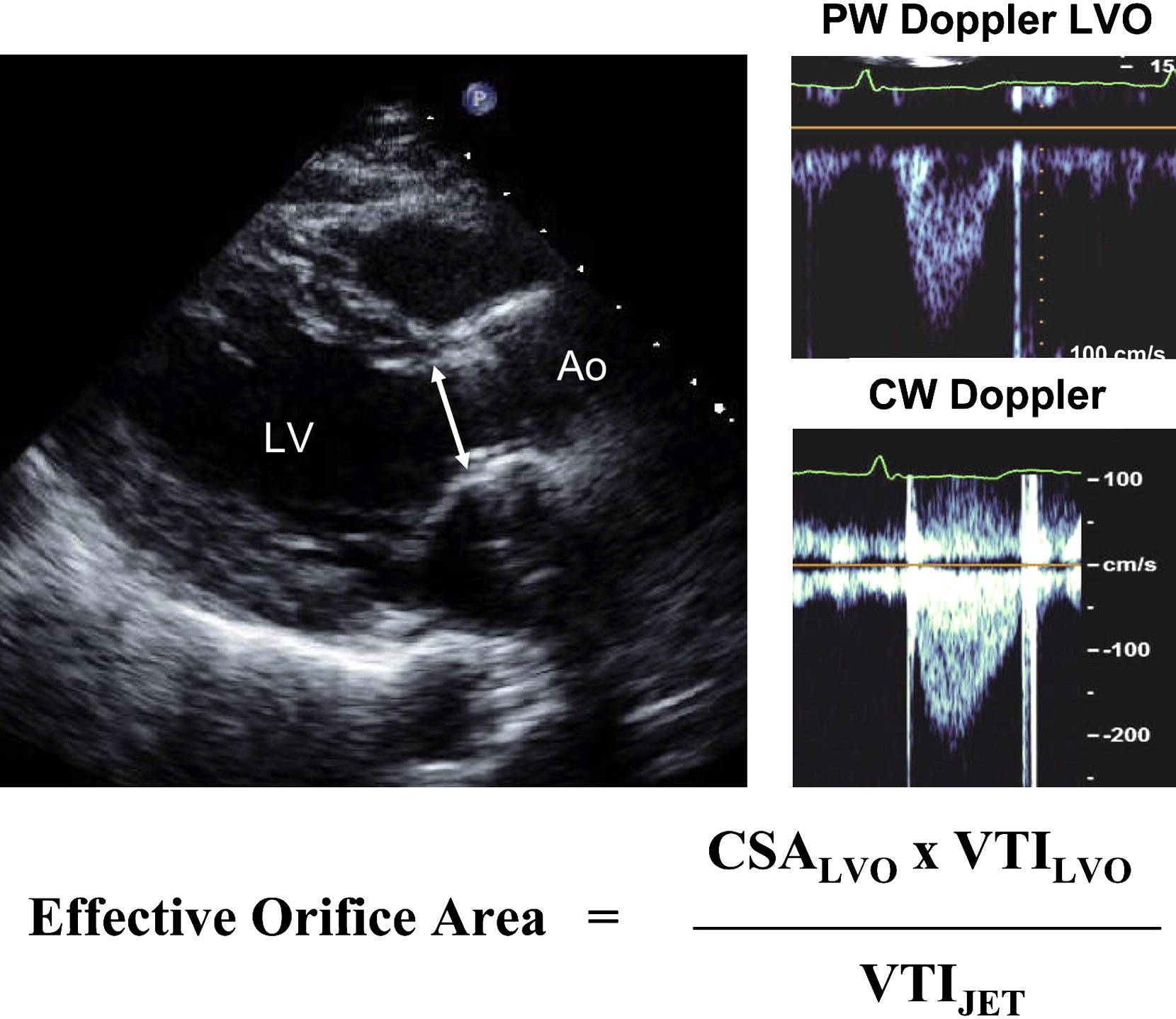
| Normal | Abnormal |
|---|---|
| > 1.2 cm2 | < 0.8 cm2 |
| < 0.6 cm2/m2 |
# Doppler Parameters for Evaluation of the Severity of Prosthetic Aortic Valve Regurgitation 评价人工主动脉瓣反流严重程度的多普勒参数
| Doppler Parameters (Qualitative or Semi-Quantitative) | ||||
|---|---|---|---|---|
| Parameters | Mild | Moderate | Severe | |
Color | Jet width in central jets | Narrow | Intermediate | Large |
| Doppler Parameters (Qualitative or Semi-Quantitative) | ||||
|---|---|---|---|---|
| Parameters | Mild | Moderate | Severe | |
CW | Jet density | Incomplete or faint | Dense | Dense |
| Quantitative Parameters | Mild | Moderate | Severe |
|---|---|---|---|
| VC width (cm) | < 0.3 | 0.3-0.59 | ≥ 0.6 |
| Reg Volume (m/beat) | < 30 | 30 - 59 | ≥ 60 |
| Regurgitant Fraction | < 30% | 30 - 50% | ≥ 50% |
| EROA (cm2) | < 0.10 | 0.10 - 0.30 | ≥ 0.30 |
Note: Comparative flow measurements can be used for prosthetic aortic and pulmonic regurgitation (annulus measurement not hindered by the prosthesis) but not for prosthetic mitral regurgitation.
注:比较血流测量可用于假体主动脉瓣和肺动脉瓣反流(瓣环测量不受假体阻碍),但不能用于假体二尖瓣反流。
- Transesophageal images of a patient with perivalvular significant AR demonstrating (arrows) the extent of dehiscence and regurgitation in cross-section and diastolic flow reversal in the descending aorta.
明显瓣周漏患者的经食道图像显示(箭头)横截面和反流的程度以及降主动脉的舒张期血流逆转。 - Flow convergence in the aortic root, vena contracta, and an eccentric jet directed anteriorly in the LVO toward the septum (left upper panel) are seen.
可见主动脉根部、缩流颈和偏心性反流在 LVO 中向前,指向间隔(左上图)中的血流汇聚。 - Because of jet eccentricity, measurement of jet width to LVO diameter is not advised in this case.
由于是偏心性反流,在这种情况下不建议测量射流宽度与 LVO 直径的比值。
# Doppler Echo Evaluation of MVR 二尖瓣人工瓣膜
- Peak early velocity 峰值早期速度
- Mean pressure gradient 平均压差
- Heart rate at time of Doppler 多普勒检查时的心率
- Pressure Half-time 压力减半时间
- Doppler velocity index:
- Presence, location and severity of regurgitation
反流的存在、位置和严重程度 - Effective orifice area 有效瓣口面积
# Doppler Parameters of Prosthetic Mitral Valve Stenosis 狭窄的指标
| Normal | Possible Stenosis | Suggests Sigificant Stenosis | |
|---|---|---|---|
| Peak velocity | < 1.9 m/s | 1.9-2.5 m/s | ≥ 2.5 m/s |
| Mean gradienty | ≤ 5 mmHg | 6-10 mmHg | > 10 mmHg |
| VTIPrMV / VTILVO | < 2.2 | 2.2-2.5 | > 2.5 |
| EOA | ≥ 2.0 cm2 | 1-2 cm2 | < 1cm2 |
| PHT | < 130 ms | 130 - 200 ms | > 200 ms |

# Other Echo Evaluation
- Left and right ventricular size, function and hypertrophy
左右心室大小、功能和肥厚 - Left and right atrial size
左右心房大小 - Concomitant valvular disease
合并瓣膜疾病 - Estimation of pulmonary artery pressure
肺动脉压的估测
Previous post-operative studies when available
以前的手术后检查 (如果有)
Comparison of above parameters is particularly helpful in suspected prosthetic valvular dysfunction
对上述参数进行比较,对于疑似瓣膜功能障碍的患者尤其有用
# Evaluation of prosthetic valves
# Challenges 挑战
- Large range in what is considered normal
正常的参考范围过大 - Mean gradients produced depend on size and type of valve
产生的平均压差取决于瓣膜的大小和类型 - Shadowing may interfere with assessment of location and amount of regurgitation
阴影可能会干扰对反流位置和程度的评估
# Pannus vs Thrombus 血管翳与血栓
超声下比较难区分,需要借助其他手段
- TOE predictors of thrombus 血栓
- Mobile mass 移动的团块
- Attachment to occluder/leaflets 附在裙边 / 瓣叶上
- Elevated gradient (peak AVR> 50mmHg, mean MVR > 10mmHg) 压差升高
- Sub therapeutic INRs (< 2.5)
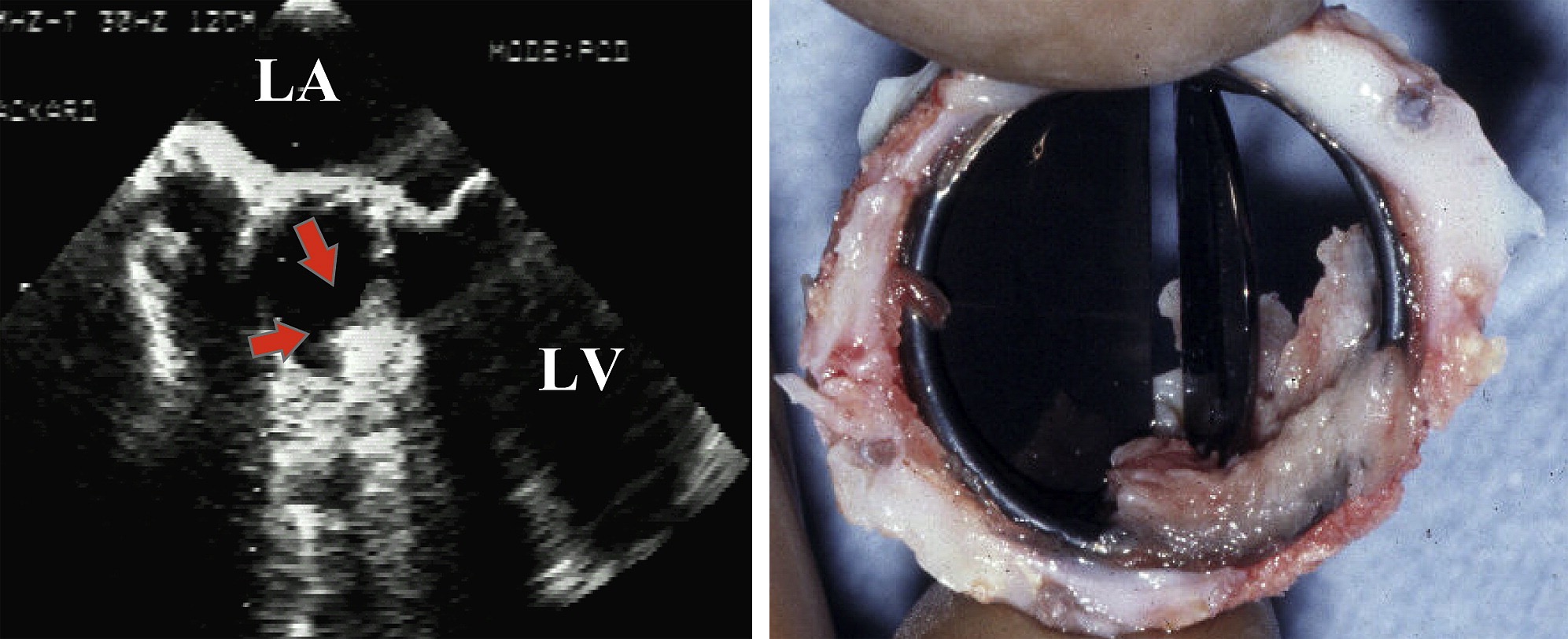
- Pannus formation on a St Jude Medical valve prosthesis in the aortic position as depicted by TEE.
如 TEE 所示,主动脉位置的 St Jude 医用瓣膜假体上的血管翳形成。 - The mass is highly echogenic and corresponds to the pathology of the pannus at surgery. The pannus is depicted by the arrows.
团块呈强回声,与手术中血管翳的病理学特征相符。血管翳如箭头所示。
# Immediate Surgical Attention 需要立即手术治疗的情况
- Risk of geometric mismatch 几何学不匹配的风险
- Moderate to severe valvular regurgitation 中度至重度瓣膜返流
- Significant paravalvular leak 严重的瓣周漏
- 'stuck' mechanical valve leaflets 机械瓣瓣叶卡住
- Valve dehiscence 瓣膜裂开
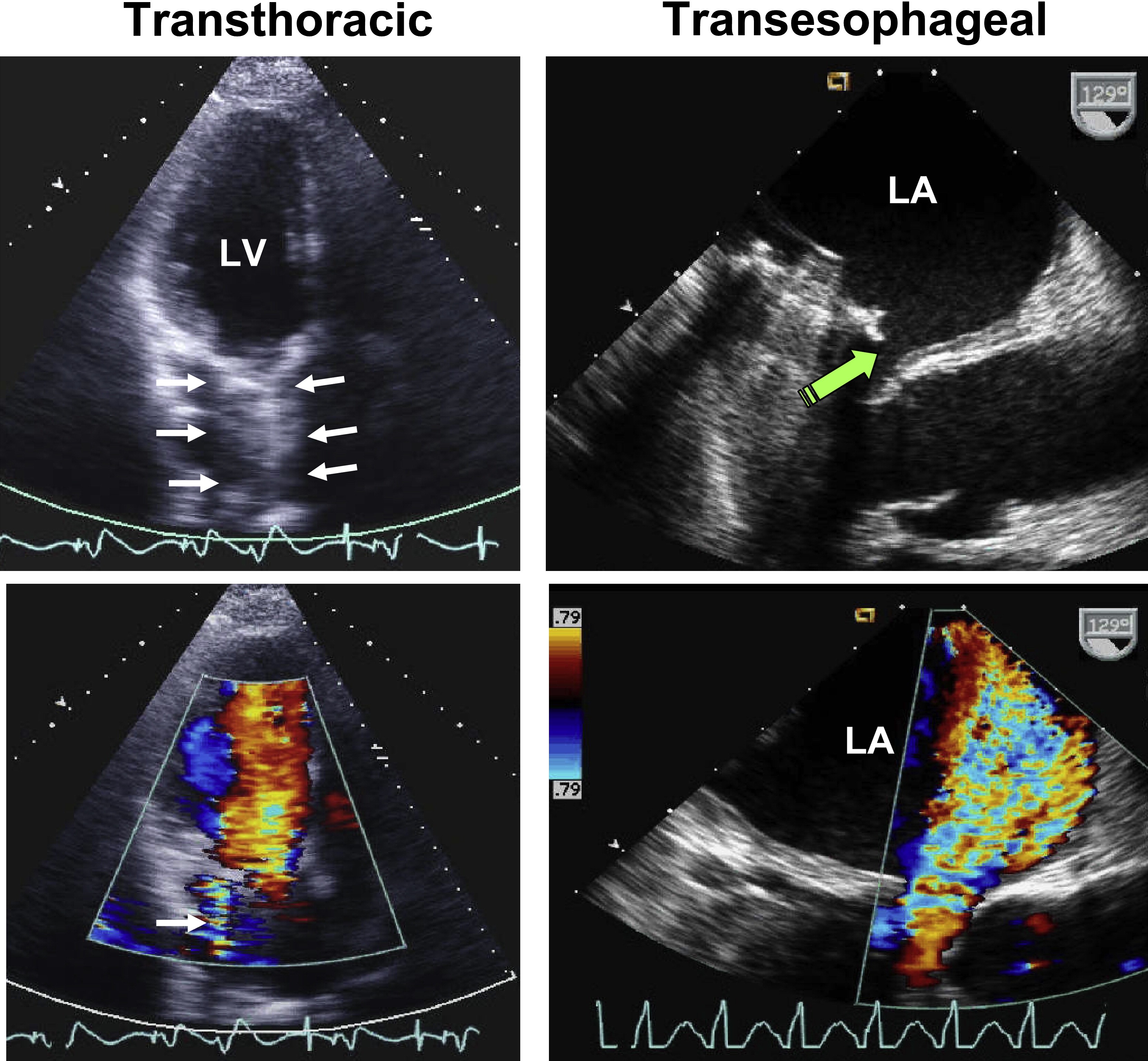
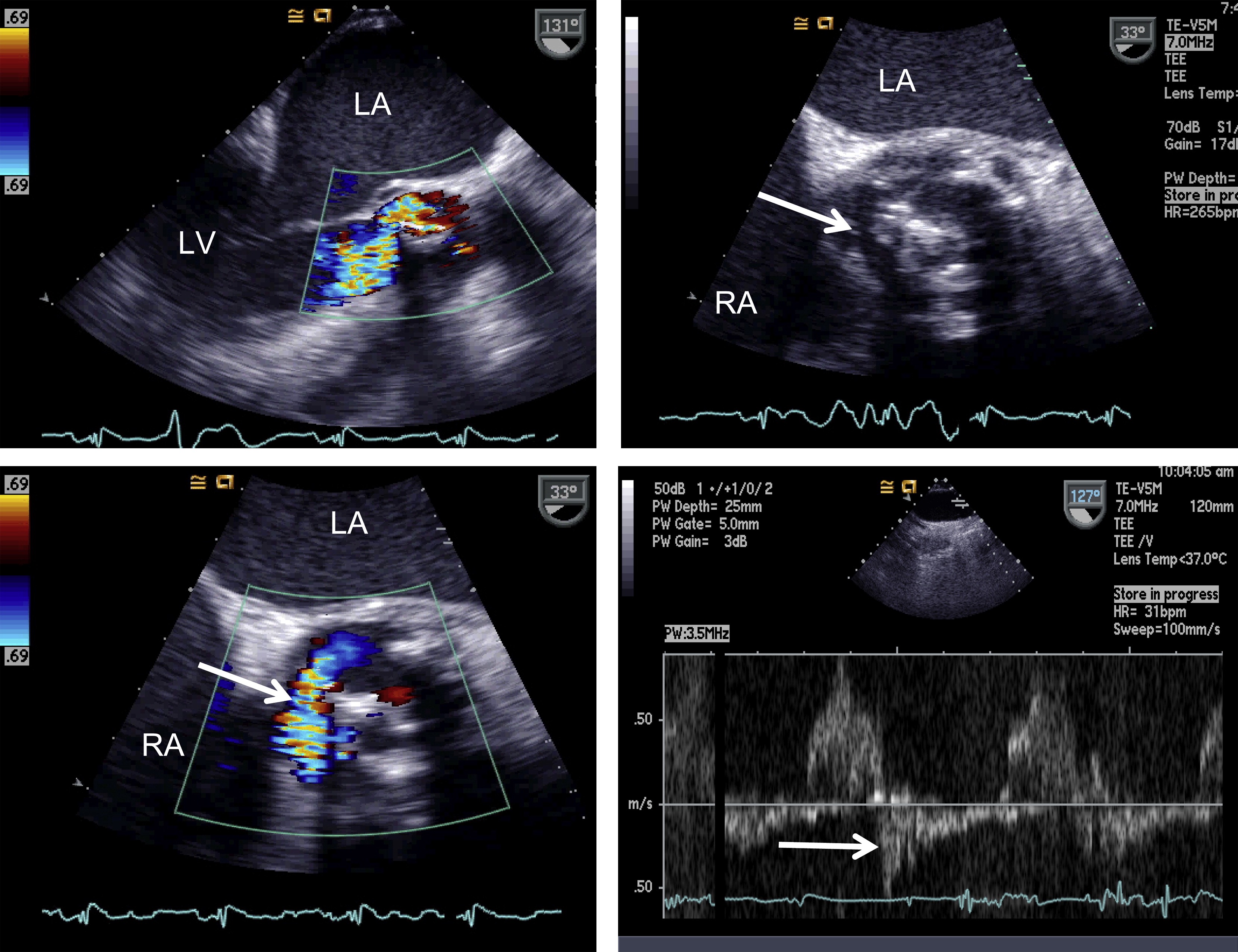
- Transthoracic versus transesophageal echocardiographic and Doppler images in a patient with severe paravalvular MR.
严重瓣周 MR 患者的经胸超声心动图和经食管超声心动图和多普勒图像。 - Shadowing on TTE of the left atrium (arrows) masked significantly the regurgitant jet by color Doppler (single white arrow).
左心房 TTE 上的阴影(箭头)通过彩色多普勒(单白色箭头)显着掩盖了反流束。 - The extent of valvular dehiscence is shown by the green arrow on TEE as well as the severity of regurgitation by color Doppler.
瓣膜裂开的程度由 TEE 上的绿色箭头表示,反流的严重程度由彩色多普勒表示。
Pibarot, P., & Dumesnil, J. G. (2009). Prosthetic heart valves: selection of the optimal prosthesis and long-term management. Circulation, 119(7), 1034–1048. ↩︎
Zoghbi WA, Chambers JB, Dumesnil JG, et al. Recommendations for evaluation of prosthetic valves with echocardiography and Doppler ultrasound. J Am Soc Echocardiogr 2009;22:975–1014. ↩︎ ↩︎