# Mitraclip
# 适应症
- Mitral regurgitation prevalence increases with age
二尖瓣反流患病率随年龄增长而增加 - Primary and secondary MR
原发性和继发性 - Patients unsuitable for surgery include:
不适合外科手术的患者包括:- Age, co-morbidities, LV dysfunction
年龄、合并症、左心室功能 - High surgical risk
外科手术风险高
- Age, co-morbidities, LV dysfunction
- Surgical options include via central sternotomy and minimally invasive surgery
外科手术包括胸骨正中切开术和微创手术 - Those without operation face recurrent hospital admissions with heart failure.
因没有手术而反复心力衰竭住院的人
# 原理
- Reducing the orifice area reduces the regurgitant volume
减少瓣口面积可以减少反流量 - Performed via a femoral venous puncture
经股静脉穿刺进行 - Transseptal puncture
房间隔穿刺 - Steerable guide catheter then positioned toward the valve
可操纵导管 SGC 朝着瓣膜进行定位 - Clip then advanced through the valve and brought back up to grasp leaflets
夹子越过瓣膜,并回撤抓住瓣叶
# 器械
- 4mm wide cobalt/chromium implant with 2 arms
4 毫米宽的钴 / 铬植入物,带两个臂 - Arms covered by polyester fabric
两个臂由聚酯纤维织物覆盖 - When open 2cm span
打开时跨度为 2 厘米 - Use 120degree view on TOE
经食道超声使用 120° 切面 - Prior to deployment check no MS
释放前检查确认没有二尖瓣狭窄 - LVESD < 70mm; LVEF 20-50%; PASP < 70mmHg; MV orifice area < 4cm2.
筛查要求

# Clinical trails
# EVEREST study. Feldman et al. JACC 2009 [1]
Table 1. Key Eligibility Criteria and Key Exclusion Criteria
- Key inclusion criteria
- Candidate for mitral valve repair or replacement surgery
- Moderate to severe (3+) or severe (4+) chronic mitral valve regurgitation and symptomatic with LVEF > 25% and LVID-s ≤ 55 mm or asymptomatic with 1 or more of the following:
- LVEF > 25% to 60%
- LVID-s ≥ 40 to 55 mm
- New onset of atrial fibrillation 新发心房颤动
- Pulmonary hypertension defined as pulmonary artery systolic pressure >50 mmHg at rest or >60 mmHg with exercise. 肺动脉高压定义为静息时肺动脉收缩压 > 50 mmHg 或运动时 > 60 mmHg。
- Key exclusion criteria
- Recent myocardial infarction 近期心肌梗塞
- Any interventional or surgical procedure within 30 days of the index procedure 手术后 30 天内的任何介入或外科手术
- Mitral valve orifice area <4 cm2 瓣口面积
- Renal insufficiency, endocarditis, rheumatic heart disease 肾功能不全、心内膜炎、风湿性心脏病
- Previous mediastinal surgery in the first 27 patients

- Result
- 107 patients - 79% primary and 21% secondary MR
107 患者 - 79% 原发性和 21% 继发性 MR - 9% had a MACE(major adverse cardiovascular events), 9% had partial clip detachment
9% 有主要心血管事件,9% 部分夹子脱落 - 74% procedural success, 64% discharged free of MR
74% 的手术成功,64% 的患者无 MR 出院 - 30% had MV surgery in the following 3 years
30% 的人在接下来的 3 年内接受了外科手术 - 2 clips placed in 29%
29% 植入了两枚夹子 - 66% of treated pts free of death, > moderate or MV surgery at 12 months
66% 接受治疗的患者在 12 个月时无死亡、无中度以上或外科手术 - Similar results between primary and secondary MR
原发和继发性 MR 之间的结果相似
- 107 patients - 79% primary and 21% secondary MR

- This chart shows the flow of patients from the point of clip procedure attempt through hospital discharge.
此图表显示了从尝试钳夹术到出院的患者流。 - Acute procedural success (APS) is defined as placement of 1 or more clips resulting in a discharge mitral regurgitation (MR) severity of ≤2+, as determined by the Core Laboratory.
即刻手术成功 (APS) 定义为放置 1 个或更多个夹子,导致出院时二尖瓣反流 (MR) 严重程度 ≤ 2+,由核心实验室确定。
# EVEREST study II. NEJM. Feldman et al. 2011 [2]

First randomised controlled trial of mitraclips but not blinded
首次随机对照试验,但非盲法Assigned 279 patients with moderate/severe 3+ or severe 4+ MR
入选了 279 名中重度 3+ 或重度 4+ MR 患者Primary end point for efficacy was freedom from death, from surgery for MV disease, from grade 3+/4+ MR
主要疗效终点是免于死亡、二尖瓣外科手术以及 3+/4+ MRPrimary end point for safety was MACE at 30d - death, MI(Myocardial infarction), re-operation, stroke, renal failure, AF, transfusion.
主要安全终点是 30d 时的主要心血管事件 - 死亡、心肌梗死、再手术、中风、肾衰竭、AF、输血。Result
- Of the total 178 in the percutaneous group, 23% had grade 3/4 MR prior to discharge and were referred for surgery
在经皮组的 178 人中,23% 的人在出院前有 3/4 级 MR,并被转诊进行外科手术 - Causes included leaflet tears post clip, failure of attachment to both leaflets
原因包括夹持后瓣叶撕裂,两个瓣叶均未夹持 - 20% in percutaneous group needed surgery vs 2% in surgery group
经皮组 20% 需要再次外科手术,而手术组为 2% - At 12 months rates of primary end point for efficacy was 55% in percutaneous-repair, and 73% in surgery (p=0.007)
在 12 个月时,经皮修复的主要疗效终点比率为 55%,手术的主要疗效端点比率为 73%(p=0.007) - At 1 month, rates of MACE were 15% in percutaneous group and 48% of pts in surgery group.
1 个月时,经皮组 MACE 发生率为 15%,手术组为 48%。
- Of the total 178 in the percutaneous group, 23% had grade 3/4 MR prior to discharge and were referred for surgery

- Subgroup analysis showed >70yos and those with functional MR had non-inferior efficacy outcomes with clips.
亚组分析显示 > 70 岁、功能性 MR 的患者在钳夹术中具有非劣效的疗效结果。
# MITRA-FR trial. Obiada et al. NEJM. 2018 [3]
- Mitraclip and medical therapy to medical therapy alone in pts with severe secondary MR
选择严重的继发性 MR 患者,分组为 MitraClip + 药物治疗和单独药物治疗组 - 12 months and 304 pts
12 个月,入选 304 位患者 - Optimised on medical therapy during the trial
试验期间对药物治疗进行了优化 - EROA 31mm2 on average and LVEDV of 135ml/m2
平均 EROA 为 31 mm2,LVEDV 为 135ml/m2 - 52% of patients with EROA < 30mm2
其中 52% 的患者 EROA < 30mm2 - No difference in rate of death or unplanned hospitalisation for heart failure
结果:心力衰竭的死亡率或计划外住院率没有差异,令人失望的结果
# COAPT trial. Stone et al. NEJM. 2018 [4]
- Mitraclip and medical therapy to medical therapy alone in pts with mod/severe or severe secondary MR
Mitraclip + 药物治疗和单独药物治疗,对中重度或重度继发性 MR 的患者 - Not suitable for open surgery due to high risk
由于高风险,不适合外科手术 - 24 months and 614 patients. 78 sites. 60% ischaemic MR
24 个月,614 名患者。78 个地点。60% 为缺血性 MR - Already on OMT
已经行优化的药物治疗 - EROA 41 mm2 on average;LVEDV of 101 ml/m2; LVEDD 6.2 cm; EF 31%
基线情况:EROA 平均 41 mm2;LVEDV 为 101 ml/m2;LVEDD 6.2 cm;EF 31% - Primary effectiveness endpoint - Hospitalisations for heart failure at 24 months
主要疗效终点 - 24 个月时因心力衰竭住院治疗 - Primary safety endpoint - Freedom from device-related complications at 12 months.
主要安全终点 - 12 个月时无器械相关并发症。


Result:
- Hospitalisations for heart failure in device group was 35.8% VS 67.9% in control group. Hazard ratio of 0.53 - CI 0.4 to 0.7 (P<0.001)
器械组的心力衰竭再住院人数为 35.8%,对照组为 67.9%。 - Death from any cause in 24 months in 29.1% in device group and 46.1% in control group. Hazard ratio of 0.62 - CI 0.46-0.82 (P<0.001)
在 24 个月内全因死亡的患者中,器械组为 29.1%,对照组为 46.1%。 - Improvement in hospitalization for heart failure and cause mortality after 24 months
24 个月后因心力衰竭再住院和全因死亡的改善 - NNT(number needed to treat) was 3.1 to prevent a hospitalisation and 5.9 to prevent death.
预防再住院的治疗人数为 31%,预防死亡的人数为 59%。
- Hospitalisations for heart failure in device group was 35.8% VS 67.9% in control group. Hazard ratio of 0.53 - CI 0.4 to 0.7 (P<0.001)
Differences 区别
- Lower EROA in Mitra-FR
- Higher LVEDV in Mitra-FR
- Lower procedural success - Cases of significant residual MR were higher in the Mitra-FR group (17% at 1yr vs 5%)
手术成功率较低 - Mitra FR 组 MR 明显残留的病例较高(1 年时 17% vs 5%)
Patient selection 患者选择
- Symptomatic and on good medical therapy
对症治疗和良好的药物治疗 - Severe MR with EROA > 40mm2
EROA > 40mm2 的严重 MR
- Symptomatic and on good medical therapy
# Specific imaging characteristics for Mitraclip 成像特征
# Optimal patient choice 最佳患者选择
- Coaptation length > 2mm; depth < 11mm
- Flail gap < 10mm; flail width < 15mm
- MV orifice area > 4cm2
- Central MR between A2/P2 ideal as less chords
- Minimal leaflet calcification; at least 5mm of distal mitral leaflet tip without calcification
二尖瓣瓣叶远端至少 5 mm 无钙化 - LVESD < 70mm
Rules can be bent as experience grows.
 anatomy measurements for suitability for MitraClip")
A. Shows how to measure flail gap which is the maximum height the prolapsing segment raises into the left atrium, measured as the distance from its opposing segment (in this case A2), red arrow, measures 7 mm - White arrow depicts length of posterior MV leaflet and measures 13 mm [5]
如何测量连枷间隙、瓣叶长度
B. Depicts 3D measurement of the maximum MV orifice in diastole - The bottom left panel shows the traced MV orifice (measures 4.8 cm2)
舒张期测量瓣口开口面积
C. Mitral annular plane (white dotted line) - When the MV closes in systole, the coaptation height is white solid line
二尖瓣瓣环,收缩期,对合高度
D. Depicts flail width
连枷宽度
E. Coaptation length, which is the degree of overlap of the leaflets along the point of coaptation.
对合长度的测量
# Defining secondary severe mitral regurgitation 继发性 MR 的定义
- AHA - EROA 0.4cm2 and RV 60mls/beat is more specific
- ESC - EROA 0.2cm2 and RV 30mls/beat
- TOE is the best modality to assess clearly and look for eccentric jets
TOE 是清楚评估和寻找偏心性反流的最佳方法 - NB the PISA method is only valid when geometric assumptions are as accurate as possible.
注意,只有当几何假设尽可能准确时,PISA 方法才有效。
# Procedure
# Transseptal puncture
- Aim for posterosuperior aspect of the fossa
卵圆窝的后上部 - Use 0 degree view for this
0° 切面 - Also, check 30-degree and bicaval view (110) in x plane
x plane 上的 30 度和双腔切面(110) - Height of 4cm above the mitral annulus in mid systole for degenerative MR and 3-4cm for secondary MR
穿刺高度,退行性 MR 位于二尖瓣环上方 4 cm,继发性 MR 位于二尖瓣环上方 3-4 cm - Once delivery sheath is in septum, switch to 120 degree view and x plane to commissural view at 60 degrees
鞘管穿过间隔,切换到 120 度切面和 xplane 60 度的交界联合切面。 - Can also use 3D view for positioning of valve.
也可以使用 3D 视图来定位瓣膜
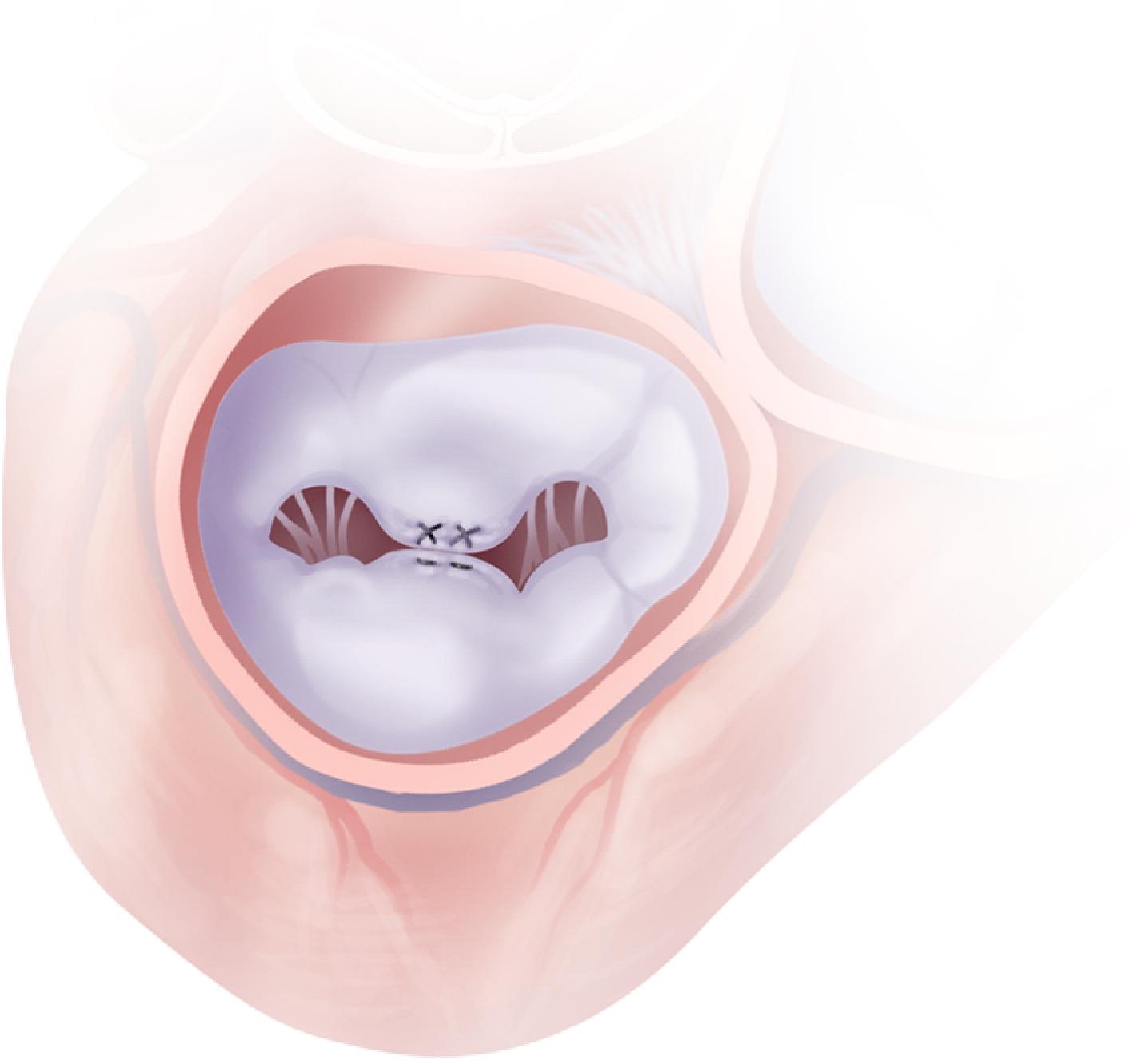
# Clipping procedure
- Arms are closed at the start and clip is lowered into optimal position [6]
夹臂在开始时关闭,降低到最佳位置 - Must be perpendicular to the leaflets
必须垂直于瓣叶 - If A2/P2, the 120 degree view is optimal
如果是二区,120° 最佳 - Arms opened when below coaptation line, and then device lifted and arms closed once leaflet capture is confirmed
在对合线下方打开双臂,一旦确认捕获瓣叶,则回撤器械并闭合双臂 - Aiming for leaflet grasp length of 5mm.
目标是瓣叶抓取长度为 5 mm

- Can deploy as long as gradients are under 5mmHg
只要压差低于 5mmHg,就可以释放 - Check position carefully with 3D and 2D, as well as fluoroscopy
用 3D 和 2D 以及透视仔细检查位置 - In some cases, a second clip may well be needed
在某些情况下,可能需要第二个夹子 - Then, delivery sheath is withdrawn across the atrial septum with clear monitoring of the resulting atrial septal defect
然后,将大鞘穿过房间隔取出,并对由此产生的房间隔缺损进行监测 - Can consider ASD device
可以考虑 ASD 封堵
# Mitraclip XT
- Longer arms by 3mm and longer grippers than NT clip
夹臂比 NT 长 3mm,抓捕片也更长 - Easier grasping due to higher frictional elements
由于摩擦力较高,抓握更容易 - Facilitates more challenging cases, e.g. more primary pathologies can be tackled with greater flail heights, smaller orifice areas
促进更具挑战性的病例,例如,可以选择更大的连枷高度、更小的瓣口面积来解决更多的原发性疾病
# Conclusions
- Patient choice is very important
患者的选择非常重要 - Surgery does remain the best choice until experience grows
在经验增长之前,外科手术仍是最佳选择 - Medical therapy for secondary MR patients is very important
继发性 MR 患者的药物治疗非常重要 - Good support with transoesophogeal echocardiography (ideally 3D)
良好的经食道超声心动图支持 (理想的 3D) - Low threshold for use of 2 clips.
使用 2 个夹子的门槛不高
Feldman, T., Kar, S., Rinaldi, M., Fail, P., Hermiller, J., Smalling, R., Whitlow, P. L., Gray, W., Low, R., Herrmann, H. C., Lim, S., Foster, E., Glower, D., & EVEREST Investigators (2009). Percutaneous mitral repair with the MitraClip system: safety and midterm durability in the initial EVEREST (Endovascular Valve Edge-to-Edge REpair Study) cohort. Journal of the American College of Cardiology, 54(8), 686–694. ↩︎
Feldman, T., Foster, E., Glower, D. D., Kar, S., Rinaldi, M. J., Fail, P. S., Smalling, R. W., Siegel, R., Rose, G. A., Engeron, E., Loghin, C., Trento, A., Skipper, E. R., Fudge, T., Letsou, G. V., Massaro, J. M., & Mauri, L. (2011). Percutaneous Repair or Surgery for Mitral Regurgitation. New England Journal of Medicine, 364(15), 1395–1406. ↩︎
Obadia, J.-F., Messika-Zeitoun, D., Leurent, G., Iung, B., Bonnet, G., Piriou, N., Lefèvre, T., Piot, C., Rouleau, F., Carrié, D., Nejjari, M., Ohlmann, P., Leclercq, F., Saint Etienne, C., Teiger, E., Leroux, L., Karam, N., Michel, N., Gilard, M., … Mewton, N. (2018). Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. New England Journal of Medicine, 379(24), 2297–2306. ↩︎
Stone, G. W., Lindenfeld, J., Abraham, W. T., Kar, S., Lim, D. S., Mishell, J. M., Whisenant, B., Grayburn, P. A., Rinaldi, M., Kapadia, S. R., Rajagopal, V., Sarembock, I. J., Brieke, A., Marx, S. O., Cohen, D. J., Weissman, N. J., & Mack, M. J. (2018). Transcatheter Mitral-Valve Repair in Patients with Heart Failure. New England Journal of Medicine, 379(24), 2307–2318. ↩︎
Rana, B. S., Calvert, P. A., Punjabi, P. P., & Hildick-Smith, D. (2015). Role of percutaneous mitral valve repair in the contemporary management of mitral regurgitation. Heart, 101(19), 1531–1539. ↩︎
Katz, W. E., Smith, A. J. C., Crock, F. W., & Cavalcante, J. L. (2017). Echocardiographic evaluation and guidance for MitraClip procedure. Cardiovascular Diagnosis and Therapy, 7(6), Article 6. ↩︎