# Aims and objectives
- To understand the basic principles of echocardiographic quantification of valve disease
了解超声心动图定量诊断心脏瓣膜病的基本原理 - Morphological techniques 形态学技术
- Assessment of valve stenosis 瓣膜狭窄的评估
- Measurement of valve gradient by Doppler echocardiography 多普勒超声心动图测量跨瓣压差
- Calculation of valve area 瓣膜面积的计算
- Assessment of valve regurgitation 瓣膜反流的评估
- Colour flow mapping and semi-quantitative techniques
彩色血流图与半定量技术 - Quantitative techniques to assess regurgitation
评估反流的定量技术
- Colour flow mapping and semi-quantitative techniques
# How to assess cardiac valves 如何评估心脏瓣膜
# Morphological assessment - Qualitative 形态学评估 - 定性
- Valve leaflet structure 瓣叶结构
- Leaflet thickness 瓣叶厚度
- Leaflet prolapse 瓣叶脱垂
- Associated masses 相关质量
- Valve leaflet movement 瓣叶运动



- Valve structure is often very informative
瓣膜结构通常信息量很大- Mitral valve 对于二尖瓣可以有
- Valve excursion 瓣膜偏移
- Trace of valve area 描绘瓣膜面积
- Is the valve prolapsing? 瓣膜有无脱垂
- Valve area measurement by planimetry
通过平面测量法测量瓣膜面积
- Mitral valve 对于二尖瓣可以有


# Functional valve assessment - Quantitative 瓣膜功能评估 - 定量
Assess valve GRADIENT (forward flow) stenotic valves
评估狭窄瓣膜的跨瓣压差(正向血流)Assess valve regurgitation - Assess chamber pressure
评估瓣膜反流 —— 评估心腔压力Assess volume of flow - Cardiac output
评估流量 —— 心输出量Assess volume of flow - Regurgitation.
评估流量 —— 反流Modalities 方式
- Colour flow Doppler 彩色血流多普勒
- CW
- PW
Calculations 计算
- Assessment of stenosis 狭窄的评估
- Assessment of regurgitation 反流的评估
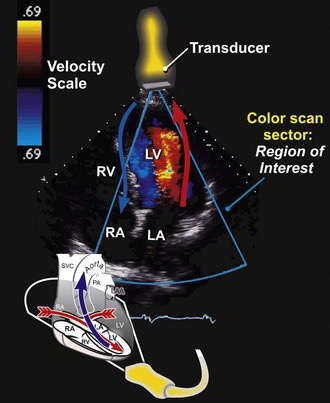
# Doppler Echocardiography
- Provides information re blood flow
多普勒提供血流信息- Direction (Colour flow mapping and spectral display)
血流方向(彩色血流图和频谱显示)- Red towards probe 红色流向探头
- Blue away from probe 蓝色远离探头
- Spectral display above or below the baseline
多普勒频谱有一个基线,如果表现在基线上方,说明血流方向是流向探头;基线以下则血流方向远离探头
- Direction (Colour flow mapping and spectral display)
- Velocity - Spectral display distance form baseline
血流速度 - 在频谱上测量基线到峰值的距离 - Amplitude - Spectral display BRIGHTNESS
振幅 - 频谱的灰度,对反流进行定性分析


- Uses 用途
- Valve assessment 瓣膜评估
- Valve gradient; valve area; regurgitation volumes
跨瓣压差;瓣膜面积;反流量
- Valve gradient; valve area; regurgitation volumes
- Stroke volume, cardiac output and intra-cardiac shunting
每搏量、心输出量和心内分流 - Estimation of LV filling pressures and diastolic function.
评估左室充盈压力和舒张期功能
- Valve assessment 瓣膜评估
# Colour Flow Mapping 彩色血流多普勒
- Multiple sample volumes along multiple scan lines
在感兴趣区域,沿多条扫描线放置了多个取样容积 - Superimposed onto real time 2D image
叠加到实时 2D 图像上 - Colour map used
使用的颜色映射 - Visual non-quantitative assessment
视觉非定量评估
# Pulsed Wave Doppler 脉冲波多普勒
- Small and spatially specific sample volume
小的有空间特异性的取样容积放置在感兴趣的区域 - Low velocities only as misreads flow direction and velocity (aliasing)
由于技术原因,比如存在误判血流方向和速度产生的混叠现象的影响,PW 仅能测量很低的速度,不像连续多普勒能测量很高的速度。 - This is because the pulse frequency is limited to allow transmission and reception of the ultrasound signal
这是因为脉冲频率被限制为允许发送和接收超声信号 - Useful to understand spatial presence of a flow
对评判空间上的某个特异点的血流状态很有用
# Continuous Wave Doppler 连续波多普勒
- Detects maximal velocity along any given line (the line of the cursor on the 2D image)
检测取样线上所有点的最大速度(2D 图像上的光标线) - Low spatial resolution
因此是低空间分辨率 - Detects high velocities
检测高速,获得最大速度(因为不知道最大速度在哪里)
实操中结合 PW 和 CW 各自的优点进行双向利用。
例如经心尖五腔心出现很高流速时,很难区分是来自左室流出道,还是来自主动脉瓣,这时根据二维形态学,以及彩色多普勒来具体观察湍流出现的部位。
还可以运用 PW 来进行特异空间点的取样,以进行区分这个最高速度大概出自哪里。

# Measure a valve gradient (Stenosis) 测量跨瓣压差(狭窄)
E.g. aortic stenosis/pulmonary stenosis:
主动脉瓣狭窄 / 肺动脉瓣狭窄- Assess highest velocity
先看二维成像 + 彩色多普勒,观察狭窄最窄的点,放置取样线
评估通过瓣膜的最高血流速度 - Ensure alignment optimized
优化取样线 cursor 位置,确保对齐平行于血流方向
CW 有角度依赖性,如果取样线有成角,结果将会被低估 - Multiple views to find highest velocities
多个切面以找到最高速度 - Use dedicated CW probe if there are poor windows.
如果视窗不好,请使用专用的 CW 探头。
也可以让患者右侧卧位
- Assess highest velocity
Views used: 使用的切面
- AORTIC: 5 chamber, 3 chamber and consider a right parasternal approach
主动脉瓣:心尖 5 腔,心尖 3 腔,考虑右胸骨旁切面 - PULMONARY: Left parasternal (SA) or subcostal
肺动脉瓣:左侧胸骨旁短轴 (SA) 或剑突下切面
- AORTIC: 5 chamber, 3 chamber and consider a right parasternal approach
# Gradient 压差
- SIMPLIFIED BERNOULLI EQUATION 简化版伯努利方程计算峰值压差


Tips and tricks
- Trace the edges of the envelope
- Avoid the hazy edges of signal
- 顶端有一些细针一样的杂波形成的模糊边缘,在描绘时应忽略、尽量避免;实际描绘时应沿着黑色部分,描计实际的清晰边缘
- 如果将模糊区域也描绘进去了,可能导致结果的狭窄严重程度被高估
BERNOUILLI EQUATION 修改版伯努利方程
- If prox velocity > 1.5m/s or Peak < 3 m/s
如果左室流出道的速度大于 > 1.5m/s 或者峰值 < 3 m/s
需要使用修改版的方程式,需要排除左室流出道的压差,用经主瓣最大血流速度减去左室流出道最大血流速度
- If prox velocity > 1.5m/s or Peak < 3 m/s
- MEAN VELOCITY = To give mean gradient TVI
平均速度 = 得出平均压差 TVI,描绘后系统会自动给出 - Used in assessment of all 4 valves
可用于评估所有四个瓣膜
# Cardiac Output 心输出量
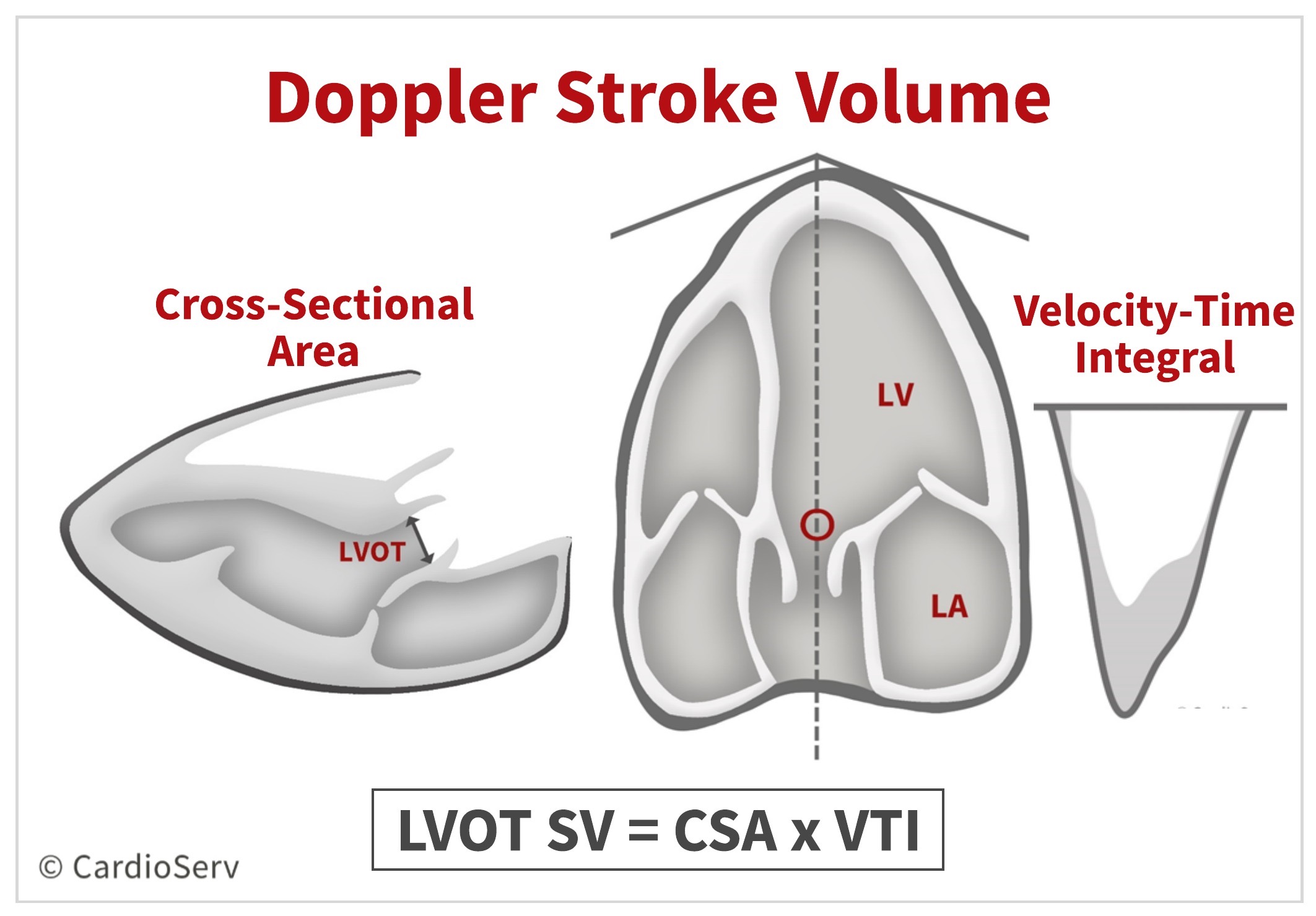
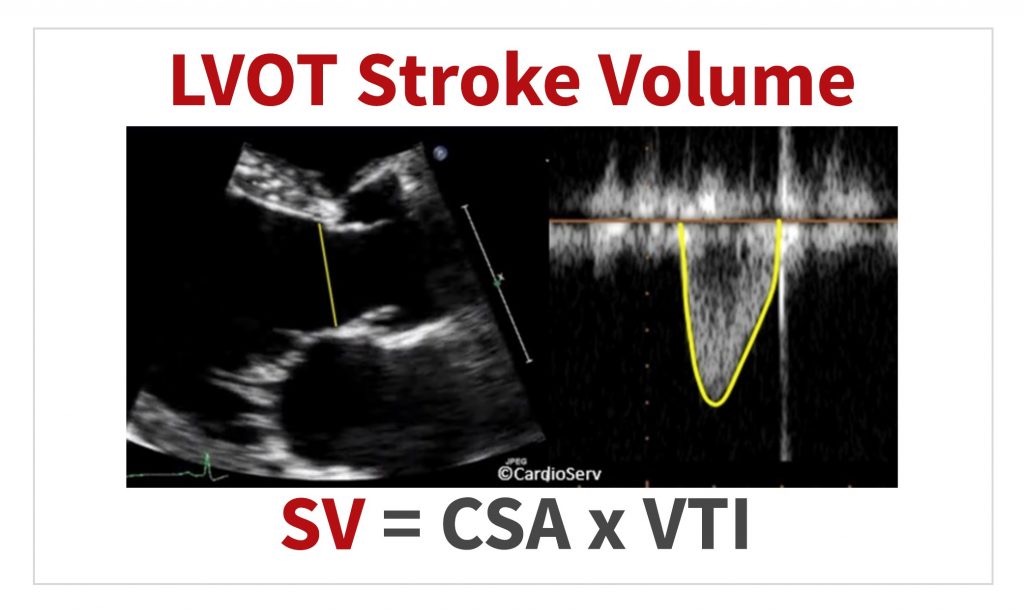
- LVOT measurements 左室流出道测量
- LVOT 直径,通过胸骨旁长轴,局部放大主动脉瓣部分进行测量
- LVOT 截面积,通过直径使用面积公式计算
- 左室流出道的速度时间积分 VTI,通过心尖五腔心,脉冲多普勒,取样容积放置在主动脉瓣上方 1cm 处,描绘频谱
- 因为 PW 具有空间特异性,取样容积放置在与胸骨旁长轴直径测量相似处,不要太靠近瓣膜。太靠近瓣膜血流会加速,因此需要适当远离瓣膜来得到很好的线性流动
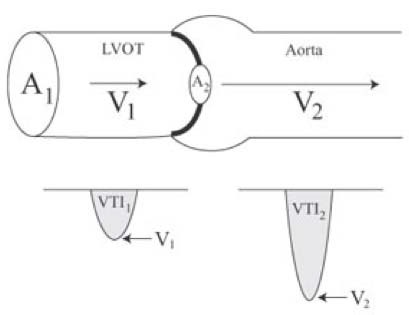
# Valve Area 瓣膜面积 - Continuity EQUATION 连续方程

- The continuity equation is based on the conservation of mass… since the volume of blood cannot be ‘lost’ – this theory supports the concept that what flows in, must flow out! In other terms: the volume proximal to valve is the same as the volume downstream from the valve. [1]
连续方程是基于质量守恒定律… 因为血量是不能 “丢失” 的 -- 这个理论支持这样一个概念,即流入的东西必须流出。换句话说:瓣膜近端的体积与瓣膜下游的体积相同。 - The stroke volume through the LVOT is equal to the stroke volume through the aortic valve.
通过左室流出道的每搏量等于通过主动脉瓣的每搏量。 - We can obtain 3 of the 4 components by calculating the stroke volume of the LVOT and measuring the peak AV velocity ( V2 ). This allows us to solve for the 4th component, which is the AVA!
通过计算左室流出道每搏输出量和测量主动脉瓣峰值速度 ( V2 ),可以得到 4 个参数中的 3 个。通过公式可以计算出第四个组成部分,即 A2 瓣膜面积 AVA!
- Tips and tricks 注意事项
- Functional area smaller than anatomical valve area
功能面积小于解剖瓣膜面积(描记法测得的值) - Major error is LVOT diameter (as it is squared):
主要误差是 LVOT 直径 (因为要按其平方计算)- Zoom view
因此需要放大测量区域 - Care on measurement point
关注测量点
- Zoom view
- Assume LVOT diameter is circular
该方法假设 LVOT 直径为圆形,但 LVOT 不一定都是圆形的,这是误差的来源之一 - Calculated either by peak or TVI velocities
面积通过峰值速度或 TVI 速度计算 - This can be used of the aortic/pulmonary valve.
连续方程式可以主动脉瓣和肺动脉瓣测量中运用 - It can also be used for mitral valve. In this case the CONTINUITY STILL APPLIES as flow in mitral = Flow through Aortic valve as long as there is no AR or MR and not AF (as stroke volume will vary so much will not be accurate).
也可以用于二尖瓣测量。应用于二尖瓣时,只要没有 AR 或 MR,没有房颤 (因为每搏量会变化多样,就不会准确),那么连续性仍然适用于二尖瓣血流 = 主动脉瓣血流。
- Functional area smaller than anatomical valve area
. The calculated EOA is smaller than the anatomical orifice area (AOA), which is the planimetry traced area.")

- As the measurement of left ventricular outflow tract (LVOT) diameter is squared in the calculation of AVA, inaccuracies in this measurement can contribute substantially to error. [2]
在计算 AVA 时,对左心室流出道 (LVOT) 直径的测量结果进行了平方运算,因此 AVA 测量结果的不准确可能会导致更大的误差。 - A combined assessment, using peak velocity, mean gradient, and the dimensionless index (simpler surrogate for aortic valve area [AVA]), provided the best sensitivity (92%) and specificity (99%) for diagnosis of severe AS compared with any single measure alone.
与任何单一测量方法相比,使用峰值速度、平均压差和无量纲指数(主动脉瓣面积的更简单替代 [AVA])的综合评估为诊断严重 AS 提供了最佳灵敏度(92%)和特异性(99%) - The dimensionless index does not depend on the measurement of LVOT diameter.
无量纲指数不依赖于 LVOT 直径的测量。 - The present study suggests routinely captured data on aortic velocities, mean gradient, and dimensionless index are more accurate than AVA in the assessment of severe aortic stenosis when compared with the clinically relevant interpretation of the echocardiographic reader.
在评估严重主动脉瓣狭窄时,常规捕获的主动脉速度、平均压差和无量纲指数的数据比直接超声描测 AVA 更准确。 - AVA, aortic valve area; CW, continuous wave; DI, dimensionless index; VTI, velocity time integral.
AVA,主动脉瓣面积;CW,连续波多普勒;DI,无量纲指数;VTI,速度时间积分。
# Valve Area 瓣膜面积 - Pressure half time 压力减半时间
There is a formula to derive mitral/ tricuspid valve area from the CW inflow
有一个公式可以从流入端 CW 得出二尖瓣 / 三尖瓣面积
可用于二尖瓣狭窄的评估The rate of decay of the velocity of flow will reflect the mitral area.
血流速度的衰减率将反映二尖瓣面积Hence, a very narrow valve will delay the return of the rate to the baseline
因此,非常窄的瓣膜将推迟速率恢复到基线的时间
# Assess Degree of Valve Regurgitation 评估瓣膜反流程度
反流的评估比狭窄困难得多
需要 Integrated Echo Assessment 综合超声评估
- Semi-quantitation/qualitative 半定量 / 定性
- Colour jet area 彩束面积
- Signal intensity 信号强度
- Pressure half time 压力减半时间
- Antegrade flow: 前向血流
- Mitral E wave in MR 二尖瓣反流中的二尖瓣 E 波
- LVOT flow in AR 主动脉瓣反流中的 LVOT 血流量
- Flow in adjacent large vessel 毗邻大血管的血流
- Pulmonary venous flow in MR 二尖瓣反流中的肺静脉血流
- Aortic flow in AR etc 主动脉瓣反流中的主动脉血流
- Quantitation: Vena contracta width, PISA
定量:缩流颈宽度,PISA - Volumetric method (Regurgitation volume /fraction)
容积法 (反流容积 / 分数) - Indirect: LA and LV size
间接线索:左房和左室大小
# Colour Doppler Assessment


| Eyeball grading of colour jet in mitral regurgitation | ||
|---|---|---|
| 二尖瓣反流中彩色射流的目测法分级 | ||
| Mild | 轻度 | 1+ |
| Moderate | 中度 | 2+ |
| Moderate to severe | 中重度 | 3+ |
| Severe | 重度 | 4+ |
Do Not Fall into Trap
- Color flow mapping is NOT an ultrasonic left ventriculogram
彩色血流图不是超声左室造影术 - Colour flow mapping is a velocity display and does not directly show volume information
彩色流图是一种速度显示,不直接显示容积信息,不能直觉的认为反流束面积 = 反流容积 - Visualised Regurgitation Jet ≠ Regurgitant volume
可视化反流束 ≠ 反流容积
- Color flow mapping is NOT an ultrasonic left ventriculogram
Factors Affecting Regurgitant Jet Area 影响反流束面积的因素
- Regurgitant volume
反流容积 - Velocity of regurgitation (driving pressure)
反流速度 (驱动压力) - Size and compliance of left atrium
左房的大小和顺应性 - Central vs wall impinging jets
中心性与偏心性的反流束 - Orifice size and shape
反流口大小和形状 - Influence of coexisting jets or flow streams
共存射流或血流的影响 - Heart rate
心率 - Technical factors.
技术因素
- Regurgitant volume
仅仅通过颜色来评估反流量可能是最危险和最不准确的方式
# CW Signal intensity 信号强度
- CW envelope 连续多普勒频谱轮廓
- The density of the CW envelope may suggest severe regurgitation:
CW 频谱的密度可能表明存在严重的返流- Dense 密集 / 灰度
- Well-defined edges 明确的清晰的边缘
- Complete envelope 完整的轮廓
- Note: Peak velocity is NOT a correlate of severity.
注:反流的峰值血流速度与严重程度无关
# Pressure half time
- Relevant to AR and PR 与主动脉瓣和肺动脉瓣反流相关
- Again, the more severe the AR the STEEPER the slope (i.e. the more severe the regurgitation, the earlier the pressure equalizes and flow reduces/stops).
同样,主动脉瓣反流越严重,频谱的坡度 / 斜率越陡峭 (即反流越严重,压力越早平衡,流动减少 / 停止) - 左室舒张末压如果升高,也会对 PHT 造成影响


# Antegrade flow 前向血流

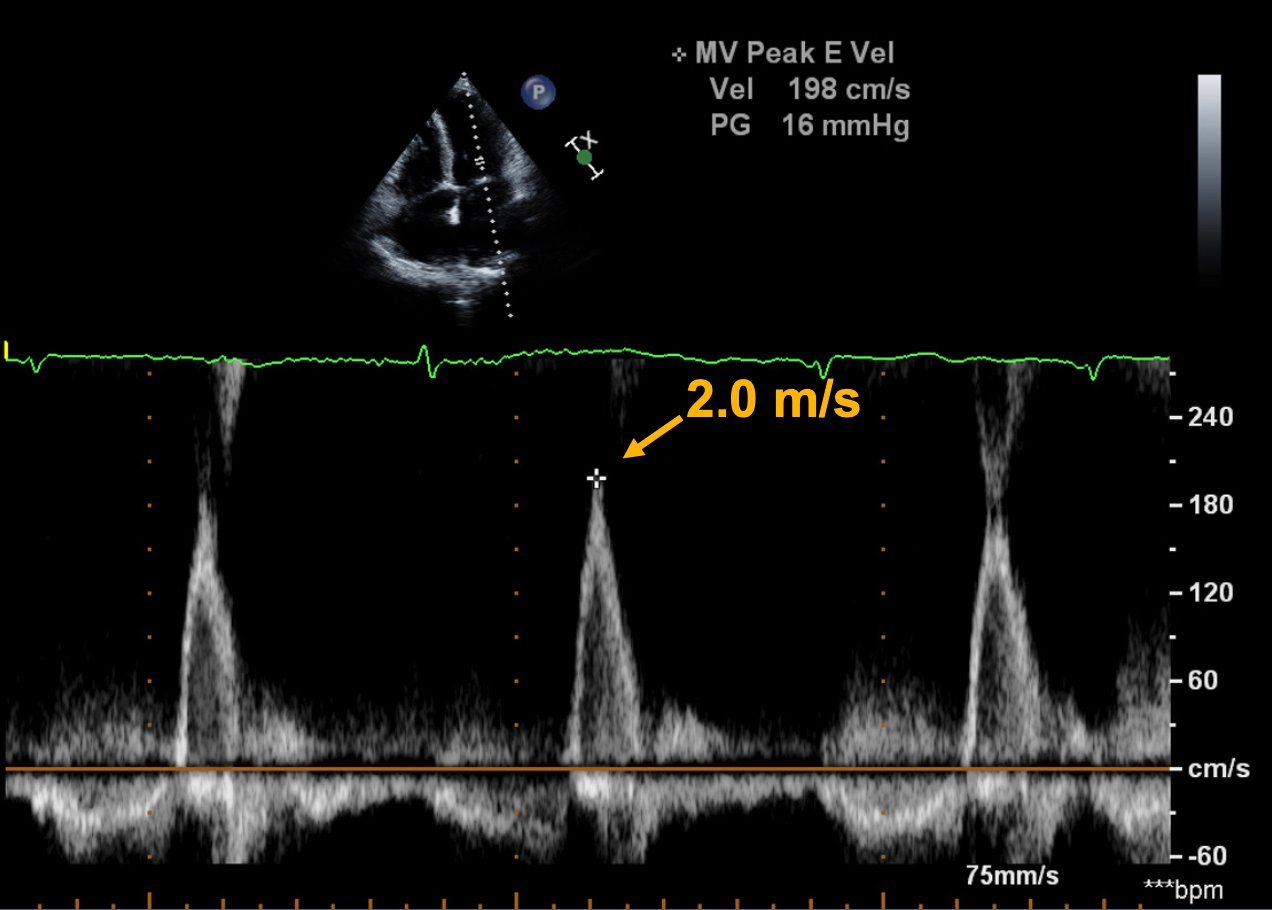
- Mitral inflow profiles showing evidence of diastolic dysfunction in dilated cardiomyopathy. [3]
扩张型心肌病患者,二尖瓣血流频谱显示舒张期功能障碍。 - The mitral inflow pulse Doppler profile in dilated cardiomyopathy often shows an impaired relaxation pattern (A) with prolonged deceleration time (DT > 200 ms) and reversal of the normal E:a ratio during the early stages.
扩张型心肌病早期,二尖瓣流入脉冲多普勒曲线通常显示舒张模式受损(A),减速时间延长(DT>200ms),正常 E:A 比值逆转。 - Later worsening of diastolic dysfunction is accompanied by a compensatory increase in left atrial filling pressures (driving pressure) results in early rapid filling of the left ventricle (a tall, thin E-wave) in the setting of a dilated left atrium.
随后舒张期功能障碍的恶化伴随着左房充盈压力 (驱动压) 的代偿性增加,导致左心房扩张时早期左心室快速充盈 (又高又细的 E 波)。 - The marked fall in the A-wave velocity reflects atrial systolic dysfunction owing to a poorly compliant left ventricle.
A 波速度的显著下降反映了左心室顺应性差导致的心房收缩功能障碍。 - Severe if E > 1.2-1.5 m/s
前向血流明显增加时,也提示二尖瓣反流程度较重 - E/A < 1 excludes severe MR
E/A<1 排除重度 MR
# Flow in adjacent vessel 邻近血管中的血流

Subcostal view: Diastolic flow reversal in abdominal aorta
剑突下切面:腹主动脉舒张期血流逆转Pulsed wave Doppler recording from the descending thoracic aorta shows forward flow in systole (above the baseline), with holodiastolic flow reversal (below the baseline and delineated by the arrows). This finding is consistent with hemodynamically significant AR.
降胸主动脉的脉冲波多普勒记录显示了收缩期的正向血流(基线以上),舒张期血流逆转(基线以下,箭头所示)。这一发现与血流动力学显著 AR 一致。
# Valve Regurgitation Quantitation 反流定量
# Jet width - Vena contracta 反流束宽度 - 缩流颈

- Vena contracta
- The small neck between the PISA region and the flair of the jet in the left atrium.
PISA 区域和左房内反流束之间的最狭窄的细颈 - Parameters Used in Grading MR Severity
MR 严重程度分级中使用的参数
- The small neck between the PISA region and the flair of the jet in the left atrium.
- 特点:
- Narrowest portion of a jet 反流束最窄的部分
- Occurs at/or just downstream from the orifice
发生在反流口 / 或恰好在反流口下游 - High velocity, laminar flow
高速,层流 - Slightly smaller than anatomic regurgitant orifice due to boundary effects
由于边界效应,比解剖反流口略小 - Represents a measure of the EROA (effective regurgitant orifice area)
表示 EROA (有效反流口面积) 的测量 - 实际操作中大部分都会测量,但也有一些复杂困难的病例不是很好测
# PISA Method (Proximal Isovelocity Surface Area) 近端等速表面积法

Hydrodynamic Principle
基于流体力学原理- As blood approaches a regurgitant orifice, its velocity increases and forms concentric, roughly hemispheric shells of increasing velocity and decreasing surface.
当血液接近反流口时,其速度增加,并形成流速递增而表面积递减的、同心的、大致为半球形的状态
- As blood approaches a regurgitant orifice, its velocity increases and forms concentric, roughly hemispheric shells of increasing velocity and decreasing surface.
PISA 利用了混叠现象,混叠速度可以通过系统设置调节,可以测得 PISA 表面的速度

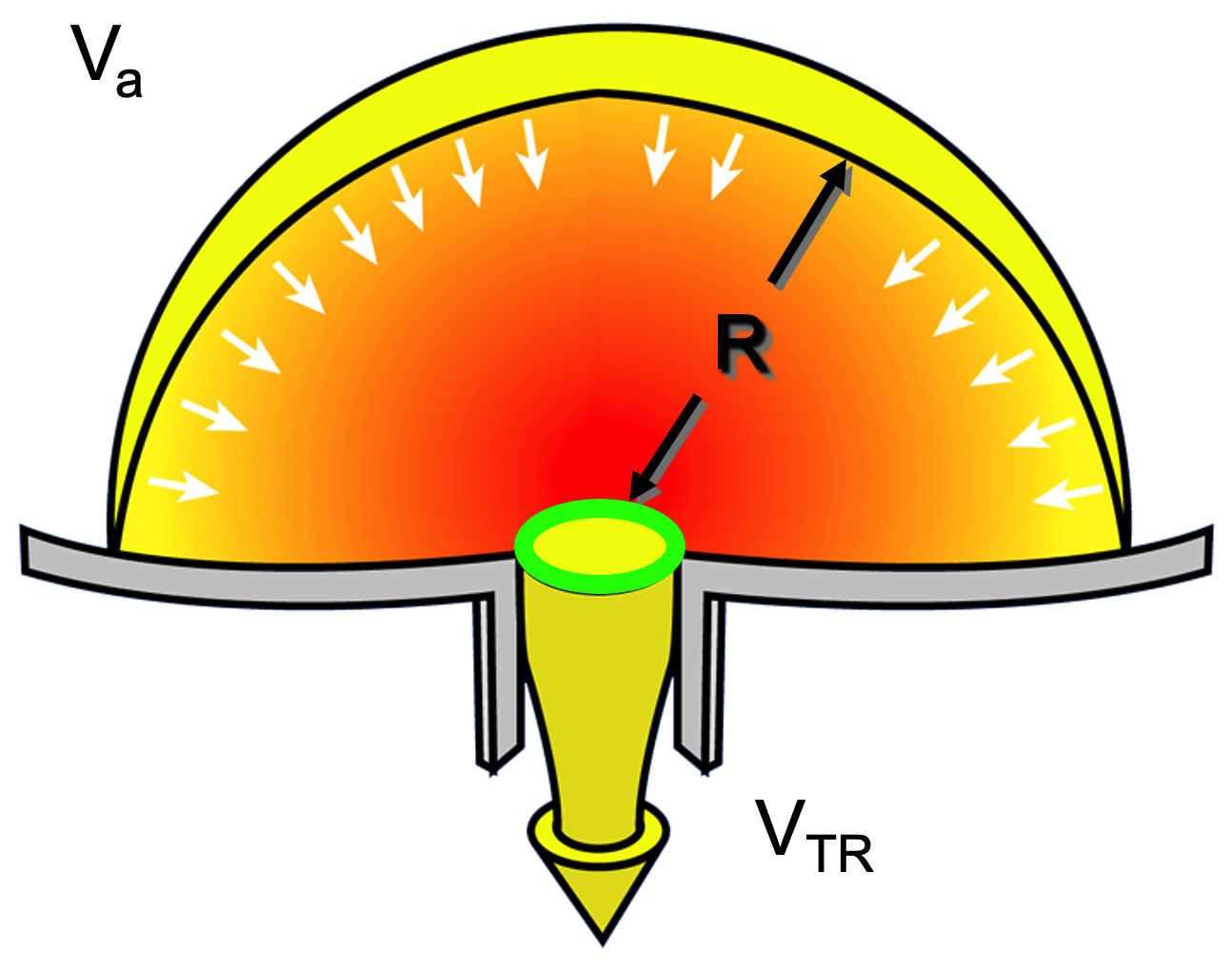
- Another form of the continuity equation
连续性方程的另一种形式- Flow entering the proximal convergence zone = Flow exiting the regurgitant orifice
进入近端会聚区的流量 = 流出反流口的流量
- Flow entering the proximal convergence zone = Flow exiting the regurgitant orifice
- Conservation of Mass / Volume 质量 / 容量守恒
- 绿色圈为 Effective Regurgitant Orifice (ERO) 有效反流口;分子为反流容积,上面已经算出;分母为二尖瓣反流最大速度,心尖四腔心切面,放置连续波多普勒,测量最大的反流速度
# Volumetric method 容积法
- If there is regurgitation in one valve, the flow volume in that valve will be higher than the non-regurgitant valve
如果一个瓣膜出现反流,该瓣膜的流量将高于无反流的瓣膜 - Hence,if MR:
# Summary
- The general principles of assessment of cardiac valve stenosis and regurgitation
- Discussion of semi-quantitative and quantitative methods
- Tips on how to avoid common errors
- Use of complementary methods to arrive at the correct diagnosis.
Aortic Stenosis: Breaking Down the Continuity Equation ↩︎
Otto CM. Heartbeat: Time to switch from aortic valve area to aortic valve index? Heart. 2019 Jan;105(2):89-91. doi: 10.1136/heartjnl-2018-314612. PMID: 30606792. ↩︎
Danik, J.S., Bulwer, B.E. (2007). Mitral Regurgitation. In: Solomon, S.D., Bulwer, B. (eds) Essential Echocardiography. Contemporary Cardiology. Humana Press. ↩︎