# Learning objectives
- Tricuspid valve anatomy 三尖瓣解剖
- Aetiology of tricuspid valve disease 三尖瓣疾病的病因
- Tricuspid regurgitation/stenosis 三尖瓣反流 / 狭窄
- Pulmonary artery pressures 肺动脉压力
# Tricuspid Valve Anatomy
- Most apical valve
更靠近心尖部的瓣膜 - 20% larger than MV annulus
比二尖瓣瓣环大 20% - Normal annulus is 3.0-3.5 cm
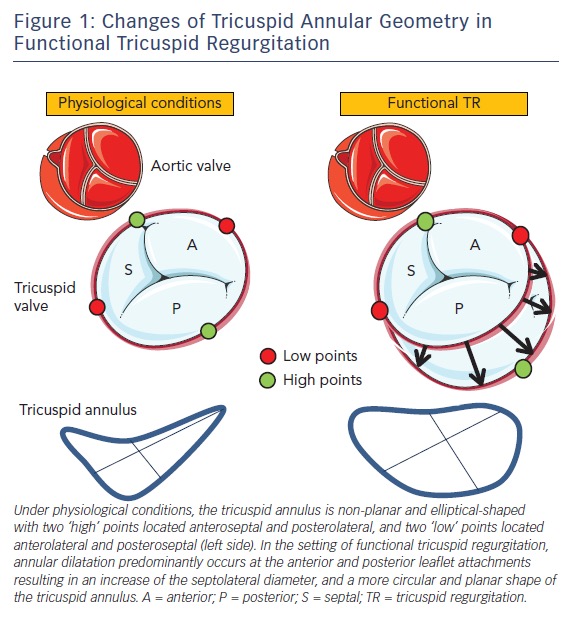
正常瓣环是 3.0-3.5 厘米 - Annular dilatation is typically at the anterior and posterior leaflet attachments
瓣环扩张通常发生在前叶和后叶附着处 - Dilatation leads to a circular annulus (causing functional TR). [1]
扩张导致圆形瓣环 (导致功能性 TR)。
- Three distinct leaflets: septal, anterior, and posterior
三种不同的瓣叶:隔叶、前叶和后叶 - The septal and the anterior leaflets are larger
隔叶和前叶较大 - Posterior leaflet is smaller and is of the least functional significance.
后叶较小,功能意义最小
: anatomical specimen and multimodality imaging. 三尖瓣(TV):解剖标本和多模态成像。")
(A) Coronal section of the heart showing TV and mitral valve and their relationships with other structures.
冠状切面显示 TV 和二尖瓣及其与其他结构的关系。
(B) Transthoracic echocardiography (TTE) four-chamber view. 经胸超声心动图(TTE)四腔切面。
(C) Transoesophageal echocardiography (TOE) four-chamber view. 经食管超声心动图(TOE)四腔切面。
(D) Three-dimensional TTE. TV leaflets and annulus from the ventricular perspective. 3D TTE。从心室面看三尖瓣瓣叶和瓣环。
AL, anterior leaflet; PL, posterior leaflet; SL, septal leaflet; TA, tricuspid annulus, chordae tendinae and papillary muscles (arrows). RA, right atrium; RV, right ventricle. [2]
- Transthoracic Views
- Parasternal RV inflow 胸骨旁右室流入道
- Apical 4 chamber 心尖四腔心
- 可以看到与二尖瓣相比,三尖瓣的瓣叶很薄,插入点更靠近心尖,这是正常的位置
- 可以看到三尖瓣的运动,对合是否良好预示着有无反流
- 可以看右房右室的大小
- Parasternal short axis 胸骨旁短轴切面
- 居中的是主动脉瓣
- 左侧约十点钟的位置是三尖瓣,上方是右室,下方是右房、房间隔
- 右侧 2-3 点钟的位置是肺动脉瓣



# Aetiology of tricuspid valve disease 三尖瓣疾病的病因
# Primary Tricuspid Valve Disease 原发性三尖瓣疾病
- Congenital 先天性
- Cleft valve - rare 瓣膜裂隙 - 罕见
- Ebstein's anomaly 埃博斯坦畸形
- Congenital tricuspid stenosis 先天性三尖瓣狭窄
- Tricuspid atresia (absent TV) 三尖瓣闭锁(三尖瓣缺失)

- Rheumatic valve disease - Leaflet thickening and fibrosis, commissural fusion, chordal fusion and shortening
风湿性瓣膜病 - 瓣叶增厚和纤维化、交界融合、腱索融合和缩短 - Infective endocarditis - Vegetation on the atrial side
感染性心内膜炎 - 心房一侧的赘生物 - Carcinoid heart disease - Endocardial fibrous thickening on the ventricular surface of the valve
类癌综合征 - 瓣膜心室侧心内膜纤维增厚 - Masses, e.g. atrial myxoma
肿块,例如心房粘液瘤 - Tricuspid valve prolapse
三尖瓣脱垂
# Secondary or Functional Tricuspid Valve Disease 继发性或功能性三尖瓣疾病
- Annular dilatation involving the anterior and posterior TV leaflets
累及前、后三尖瓣瓣叶的瓣环扩张- Right ventricular dilatation
右心室扩张 - Pulmonary hypertension
肺动脉高压 - Global RV dysfunction from cardiomyopathy/myocarditis
心肌病 / 心肌炎导致的整体 RV 功能障碍 - Segmental dysfunction due to RV ischemia or infarction, endomyocardial fibrosis, ARVC.
右室缺血或梗死、心内膜心肌纤维化、急性下腔静脉节段功能障碍、致心律失常性右室心肌病
- Right ventricular dilatation
# Key Point
Mild TR is seen in up to 60% of healthy patients
高达 60% 的健康患者可以看到轻度的 TRModerate TR in up to 15% of healthy patients.
高达 15% 的健康患者可以有中度 TRMild or moderate TR in a valve with thin leaflets, normal coaptation, and normal-appearing supporting structures is physiological or functional.
瓣叶薄、对合正常、支持结构看起来正常的,轻度或中度瓣膜反流是生理性或功能性的。
# Carcinoid 类癌
- Leaflets are thickened and retracted with a fixed orifice - Leads to a failure of coaptation
瓣叶变厚,固定的瓣口使其回缩受阻 - 导致对合失败 - Predominantly causes severe TR (severe MS less common)
主要导致严重 TR (严重 MS 较少见) - CW shows classic dagger shaped jet
CW 显示了经典的匕首状反流频谱图 - 10% have left-sided valvular pathology due to eithe high tumour load, bronchial carcinoid or PFO.
10% 的患者因肿瘤负荷高、支气管类癌或 PFO 而出现左侧瓣膜病变。
. 三尖瓣癌样病变")
- A, Right ventricular inflow view. Fixed, retracted, and thickening of tricuspid valve leaflets and associated chordae. [3]
右心室流入道切面。三尖瓣瓣叶和腱索的固定、回缩和增厚。 - B, Continuous-wave Doppler showing dagger-shaped profile of tricuspid regurgitation (TR).
连续波多普勒显示三尖瓣反流 (TR) 的匕首形轮廓。 - C, Apical 4-chamber view showing dilated right ventricle with tricuspid valve leaflets failing to coapt resulting in constant semiopen position.
心尖四腔切面显示右心室扩张,三尖瓣叶不能对合,呈恒定的半开状态。 - D, Color Doppler demonstrating severe tricuspid regurgitation into a dilated right atrium.
彩色多普勒显示严重的三尖瓣反流进入扩张的右心房。
# Ebstein's Anomaly
- Congenital 先天的
- Downward displacement of tricuspid valve
三尖瓣插入点的向下朝心尖部的位移 - Primary complication is severe TR
主要并发症是严重的 TR - The anterior leaflet is "sail like".
前叶呈 “帆状”


# TV Prolapse
- 30% with MVP have redundancy and prolapse of the TV
30% 的 MV 有三尖瓣冗余和脱垂 - Varying degrees of tricuspid regurgitation
不同程度的三尖瓣反流
# How to Assess TR Severity
- Anatomic - Tricuspid annular dilatation, valve leaflets
解剖 - 三尖瓣环扩张、瓣叶 - Right atrium and right ventricle
右心房和右心室 - Colour Flow
彩色血流 - Jet area
反流面积 - Vena Contracta
缩流颈 - Continuous Wave Doppler 连续波多普勒
- PISA/flow convergence method
- Hepatic vein flow reversal 肝静脉血流逆转
# Colour Flow 彩色血流
- Can be assessed in RV inflow, PSAX, A4C
可以在 RV 流入、PSAX、A4C 中评估 - CFM over the right atrium
彩色血流频谱覆盖在右房 - Small central jet in mild TR
小的中央性射流一般是轻度 TR - Broad central or eccentric jet with coanda effect in severe TR.
宽大的中心性的或偏心性的反流束具有柯安达效应,是重度 TR
 Large central jet; 大的中央型反流 (B) eccentric jet with a clear Coanda effect. 有明显科恩达效应的偏心性反流")
# Continuous Wave
Assessed in RV inflow, PSAX, A4C
可以在 RV 流入、PSAX、A4C 中评估CW at TR jet
在三尖瓣反流束上放置连续波多普勒Mild: faint and parabolic
轻度:柔和、抛物线状Severe: dense/triangular with early peaking (peak at < 2m/s)
重度:密集、三角形,早期达到峰值


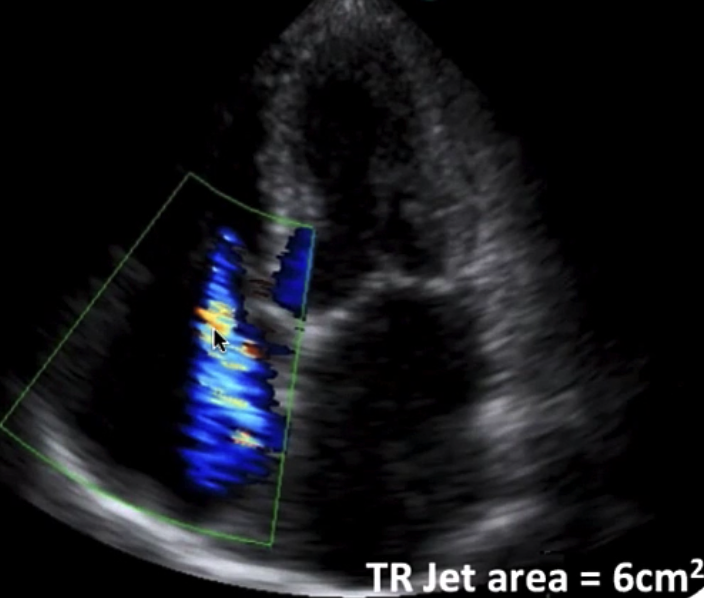
# Jet area
- Apical 4 chamber 心尖四腔心
- Perform at Nyquist limit 50-70cm/s 尼奎斯特极限的设置
- Underestimates eccentric jets and overestimates central jets.
低估偏心性反流,高估中央性反流- [important caveats] 如果偏心性反流 hugs 拥抱了房间隔或者 across 跨过了右房侧壁,可能导致偏心性反流
| Mild | Moderate | Severe |
|---|---|---|
| < 5cm2 | 5-10cm2 | > 10cm2 |
# Vena Contracta
- The point in a fluid stream where diameter is the least/narrowest and fluid velocity is at its maximal
流体中直径最小、流体速度最大的点 - Apical 4 chamber 心尖四腔心
- CFM over RA 彩色血流图放置在右房
- Nyquist limit 50-60cm/s 尼奎斯特极限
- More accurate for central TR.
对于中央型 TR 更准确
| Mild | Moderate | Severe |
|---|---|---|
| no values exist | < 7mm | > 7mm |

- Semi-quantitative assessment of tricuspid regurgitation severity using the vena contracta width (VC). The three components of the regurgitant jet (flow convergence zone, vena contracta, jet turbulence) are obtained. [4]
使用缩流颈缩宽度 (VC) 半定量评估三尖瓣关闭不全的严重程度。获得了反流束的三个组成部分 (血流会聚区,缩流颈,湍流区)。
# Proximal Isovelocity Surface Area (PISA) Radius
- Apical 4 chamber
- Zoom at TV leaflets
- Baseline to 30-40cm/s
- downward shift of zero baseline to obtain an hemispheric PISA
- Measure from vena contracta to first aliasing threshold
从缩流颈到第一个混叠区域的测量
| Mild | Moderate | Severe |
|---|---|---|
| < 0.4cm | 0.4 - 1.0cm | > 1.0cm |
 method.")
- (F) continuous wave Doppler of tricuspid regurgitation jet allowing calculation the effective regurgitant orifice area (EROA) and regurgitant volume (R Vol). TVI, time-velocity integral.
(F) 三尖瓣返流的连续波多普勒,可计算有效返流口面积 (EROA) 和返流体积 (RVol)。TVI,时间 - 速度积分。
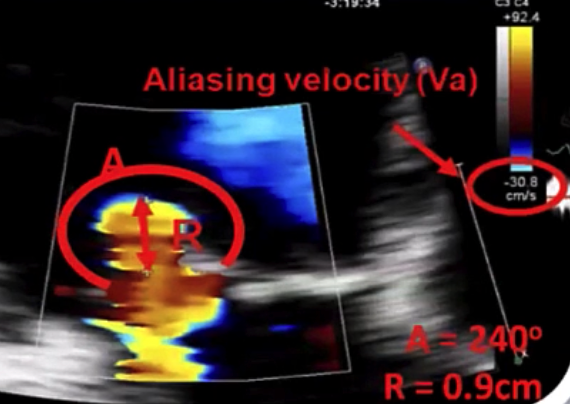
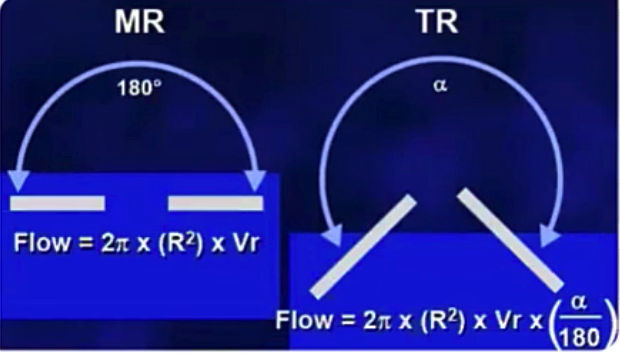
In this example PISA surface area
三尖瓣反流的 PISA 需要考虑夹角度数
# Regurgitant Flow
- In this example Regurgitant Flow
# Effective Regurgitant Orifice Area 有效返流孔口面积
- CW at TR jet to obtain TR Vmax
在三尖瓣反流束放置连续波多普勒获得 TR Vmax
- In this example
| Mild | Moderate | Severe |
|---|---|---|
| < 0.2 cm2 | 0.2-0.39 cm2 | ≥ 0.40 cm2 |
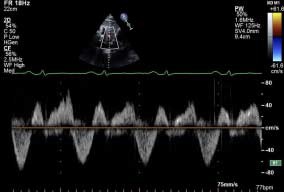
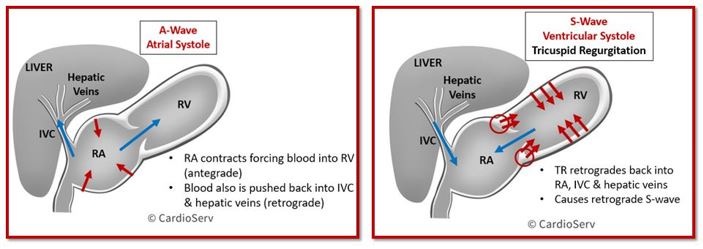
# Hepatic vein flow reversal 肝静脉血流逆转
Subcostal view 剑突下切面
Continuous wave doppler at hepatic vein.
肝静脉连续波多普勒Retrograde flow during ventricular systole in severe TR
严重 TR 心室收缩时的逆行血流


# Tricuspid Stenosis 三尖瓣狭窄
- Congenital 先天性
- Rheumatic heart disease: usually with rheumatic mitral involvement
风湿性心脏病:通常伴有风湿性二尖瓣病变 - Connective tissue: SLE, Loeffler's endocarditis
结缔组织病:系统性红斑狼疮、Loeffler 心内膜炎 - Malignant: Metastatic melanoma, carcinoid, RA mass
恶性:转移性黑色素瘤、类癌、类风湿关节炎肿块 - Infective endocarditis
感染性心内膜炎
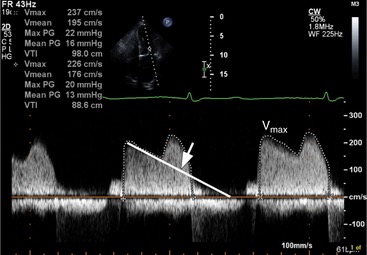
# Rheumatic Tricuspid Stenosis

Thickened leaflets with restricted motion and commissural fusion
瓣叶增厚,运动受限,交界融合Diastolic doming of the TV
舒张期三尖瓣呈穹顶样(图中左侧前叶)Right atrial dilatation
右房扩张Dilated IVC / hepatic veins
扩张的下腔静脉 / 肝静脉IAS bulging into left atrium
房间隔膨胀到左心房Mixed TS/TR
有时狭窄和反流并存
# Right Atrial Mass 右心房肿块
- Myxomas are the most common benign cardiac tumours
粘液瘤是最常见的心脏良性肿瘤。 - LA in 75%; RA in 25%
- Usually single polypoid
通常为单个息肉样 - Pedunculated and attached to IAS with short stalk
带蒂,短柄与 IAS 相连 - Can obstruct the SVC/VC or TV outflow.
会阻塞 SVC/VC 或三尖瓣流出道
# Tricuspid Stenosis Severity 三尖瓣狭窄严重程度
Continuous wave doppler : 连续波多普勒
- Mean Pressure Gradient 平均压差
- Pressure Half-Time: 压力减半时间
- PHT is not reliable when there is significant RV dysfunction or pulmonary regurgitation
当有严重的右室功能障碍或肺动脉瓣反流时,PHT 不可靠(PHT 受 PR 影响) - Significant TR will increase mean gradient.
显著的三尖瓣反流将增加平均压差
- PHT is not reliable when there is significant RV dysfunction or pulmonary regurgitation
Can be missed on routine echocardiography
常规超声心动图检查可能会遗漏Degree of leaflet thickening may appear subtle
瓣叶增厚程度可能不明显Planimetry of the tricuspid valve orifice by 2D images is difficult and unreliable
利用二维图像对三尖瓣口进行平面测量既困难又不可靠Valve area is not usually used for determining TS severity
瓣膜面积通常不用于确定 TS 严重程度TVA <1.5 cm2 is significant enough to cause symptoms.
才会引起症状(三尖瓣比二尖瓣大)
# Mean Pressure Gradient
- Apical 4 chamber or at RV inflow
心尖四腔心或右室流入道 - Continuous wave doppler at TV annulus
三尖瓣瓣环处的连续波多普勒 - Trace around the TV inflow.
对三尖瓣流入血流进行跟踪 [5]
| Mild | Moderate | Severe |
|---|---|---|
| < 2 mmHg | 2-5mmHg | ≥ 5 mmHg |


# Pressure Half Time
Apical 4 chamber or at RV inflow
心尖四腔心或右室流入道Continuous wave doppler at TV annulus
三尖瓣瓣环处的连续波多普勒Time interval in ms between the maximum tricuspid gradient and the where the gradient is half the maximum initial value
三尖瓣最大压差到最大压差的一半的时间间隔 (ms)Severe TS > 190ms
# TV Area
| Mild | Severe |
|---|---|
| > 7 cm2 | < 1 cm2 |
- 3D echocardiography can help to accurately obtain a tricuspid valve area.
三维超声心动图有助于准确获得三尖瓣面积。
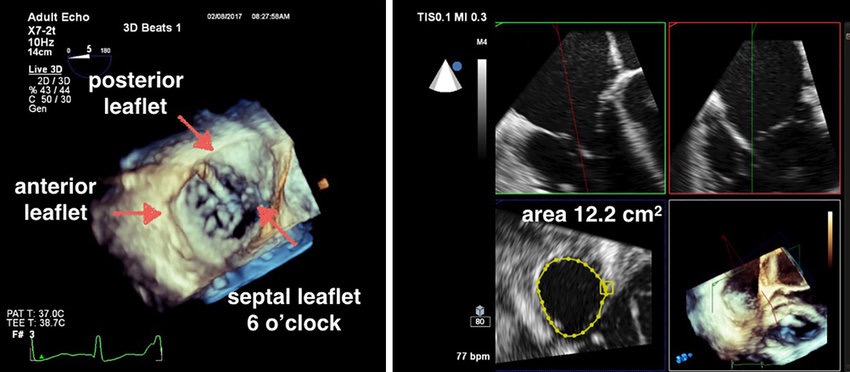
- 3D narrow sector acquisition of the tricuspid valve (TV). (A) En face view of the TV with the leaflets labeled and the orientation such that the septal leaflet is at 6 o'clock; (B) MPR with green and red plane orthogonal to the blue, short axis plan to determine the TV annular area in mid-diastole.
三尖瓣(TV)的 3D 窄扇区采集。(A) 三尖瓣正面视图,带有标签的瓣叶和方向,使隔瓣位于 6 点钟;(B) MPR 具有与蓝色正交的绿色和红色平面,短轴平面图用于确定舒张中期的三尖瓣瓣环面积。
# Calculating Right Sided Pressures 计算右侧压力
- 连续方程式
- Pressure gradient between RA and RV is the same as that between PA and RV
RA 和 RV 之间的压差与 PA 和 RV 之间的压差度相同 - Hence, in the absence of RVOT obstruction
因此,在没有 RVOT 阻塞的情况下
# Estimate Right Atrial Pressure (RAP) 右房压
- Obtain the IVC in subcostal window
剑突下切面得到 IVC 成像 - Ask the patient to sniff - mimics inspiration - and assess collapsibility of the IVC.
让病人快速吸气 - 模仿吸气,并评估下腔静脉的崩溃 / 塌陷
| 1️⃣ Size of IVC | 2️⃣ IVC size On Inspiration | Right atrial pressure(mmHg) |
|---|---|---|
| Small < 1.5cm | Near total collapse | 0 - 5 |
| Normal(1.5-2.5cm) | Decrease > 50% | 5 - 10 |
| Normal | Decrease < 50% | 10 - 15 |
| Dilated > 2.5cms | Decrease ≤ 50% | 15 - 20 |
| Both IVC & Hepatic veins dilated | No change | > 20 |
# Pulmonary Artery Systolic Pressure 肺动脉收缩压
Equal to Right Ventricular Systolic Pressure = TR max pressure gradient + Right atrial pressure
In the absence of RVOT obstruction
| Normal | Mild | Moderate | Severe |
|---|---|---|---|
| < 25 mmHg | 25 to 40 mmHg | 40 to 70 mmHg | > 70 mmHg |
# TR doppler jet
- Assessed in parasternal RV inflow, parasternal short axis or apical four chamber
在胸骨旁右室流入道、胸骨旁短轴或心尖四腔心中评估 - Continuous wave doppler at the TR jet
TR 射流处的连续波多普勒
# Bernouli Equation
- When fluid passes through a narrow space, the velocity increases.
- Pressure is increased before the obstruction and is low behind the obstruction.
- The difference between these pressures is known as the pressure gradient, which can be calculate using the Bernoulli equation.
# mPAP from PASP
- Mean pulmonary artery pressure can be estimated from PASP
- mPAP is the measurement used during right heart catheterisation
- Therefore a PASP of 40mmHg is equal to mean PAP of 25mmHg
因此,40mmHg 的 PASP 等于 25mmHg 的 mPAP - Can also calculate the mPAP using pulmonary flow dopplers.
也可以使用肺血流多谱勒计算 mPAP
# PV Acceleration Time 肺动脉瓣加速时间
- Can use the PV acceleration time in isolation to estimate pulmonary pressures
可以单独使用肺动脉瓣加速时间来估计肺动脉压 - Time between onset of flow and max velocity (ms):
从血流开始到达到最大速度之间的时间 (ms)
| Normal | Borderline 临界 | Confirmed | Severe |
|---|---|---|---|
| > 130ms | 100 - 130ms | 80 - 100ms | < 80ms |
# dPAP or mPAP from PR Jet
三尖瓣反流不显示,或者频谱图无法完整显示时
Assessed using continuous wave doppler in the PSAX window at the RV outflow
在 RV 流出道的 PSAX 窗口中使用连续波多普勒进行评估Line up with the PR jet
取样线与肺动脉瓣反流平行肺动脉舒张压
- 平均肺动脉压
Besler, C., Meduri, C. U., & Lurz, P. (2018). Transcatheter Treatment of Functional Tricuspid Regurgitation Using the Trialign Device. Interventional Cardiology (London, England), 13(1), 8–13. ↩︎
Ancona, F., Stella, S., Taramasso, M., Marini, C., Latib, A., Denti, P., Grigioni, F., Enriquez-Sarano, M., Alfieri, O., Colombo, A., Maisano, F., & Agricola, E. (2017). Multimodality imaging of the tricuspid valve with implication for percutaneous repair approaches. Heart (British Cardiac Society), 103(14), 1073–1081. ↩︎
Bhattacharyya, S., Davar, J., Dreyfus, G., & Caplin, M. E. (2007). Carcinoid Heart Disease. Circulation, 116(24), 2860–2865. ↩︎
Lancellotti, P., Moura, L., Pierard, L. A., Agricola, E., Popescu, B. A., Tribouilloy, C., Hagendorff, A., Monin, J.-L., Badano, L., Zamorano, J. L., on behalf of the European Association of Echocardiography, Document Reviewers:, Sicari, R., Vahanian, A., & Roelandt, J. R. T. C. (2010). European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: Mitral and tricuspid regurgitation (native valve disease). European Journal of Echocardiography, 11(4), 307–332. ↩︎
Saxena, A. (2013). Echocardiographic Diagnosis of Chronic Rheumatic Valvular Lesions. Global Heart, 8(3), 203–212. ↩︎