# Learning objectives
- How to assess MR Severity
如何评估 MR 严重程度 - Colour Flow measures
彩色血流 - Doppler methods of MR assessment
多普勒 - PISA/flow convergence and limitations
近端等速表面积 / 血流收敛方法及其局限性 - Volumetric assessment and limitations
容量评估及其局限性 - Role of special tests in MR
其他特殊检测在 MR 中的作用
# How to Assess MR Severity
- Anatomic: valve structure, LA / LV dimensions
解剖:观察瓣膜结构,左房左室大小 - semi-quantitative methods 半定量方法
- Colour Flow Mapping
彩色血流 - Jet area and Jet area / Left atrium ratio
观察反流面积,以及反流面积与左房的比值 - Vena contracta width
缩流颈宽度
- Colour Flow Mapping
- Quantitative methods
定量方法- PISA/flow convergence technique 血流汇聚技术
- Continuous wave doppler 连续波多谱勒
- Pulmonary vein flow reversal 肺静脉血流逆转
- Doppler volumetric method 多普勒容积法
- Pulsed wave E' 脉冲多普勒
# Qualitative / Semi-quantitative methods 定性 / 半定量方法
# Colour Flow


| Eyeball grading of colour jet in mitral regurgitation | ||
|---|---|---|
| 二尖瓣反流中彩色射流的目测法分级 | ||
| Mild | 轻度 | 1+ |
| Moderate | 中度 | 2+ |
| Moderate to severe | 中重度 | 3+ |
| Severe | 重度 | 4+ |
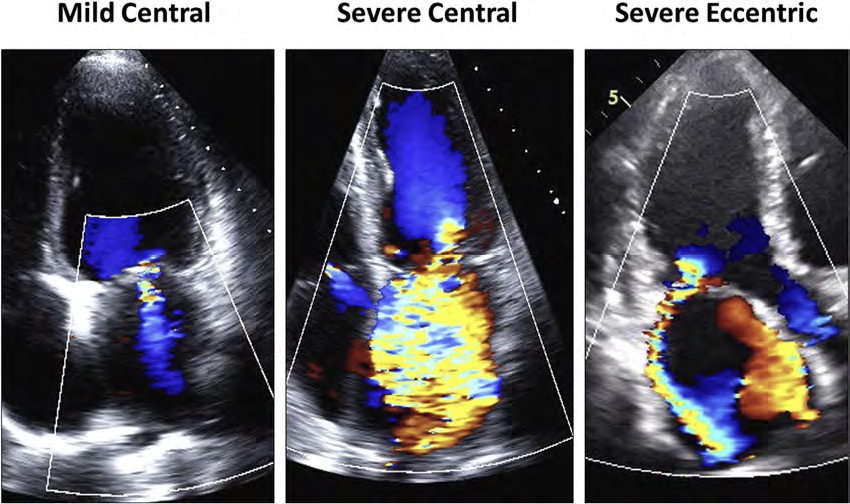
- Assessed in PLAX, A4C, A3C, A2C
在胸骨旁长轴、心尖四腔心、心尖三腔心、心尖两腔心 - colour flow mapping(CFM) over left atrium
在左房加持彩色多普勒 - Small central jet in mild MR
轻度反流为小而中心性的反流束 - Broad central or eccentric jet with coanda effect in severe MR
严重二尖瓣反流则多为具有柯恩达效应(沿物体表面的高速气流在拐角处能附于表面的现象)的宽的中心性或偏心性反流束 - Colour flow methods are only for diagnosing MR and are not for MR quantification
彩色血流法仅用于 MR 诊断,不适用于 MR 定量




# Jet area 反流束面积
- Apical 4 chamber
心尖四腔心 - Nyquist limit 50-70cm/s
尼奎斯特极限 - Planimetry around MR jet
对反流束进行平面描绘 - Underestimates eccentric jet and overestimates central jet
低估偏心性反流或小反流,高估中心性反流
| Mild | Moderate | Severe |
|---|---|---|
| < 4cm2 | 4-10cm2 | > 10cm2 |
# Jet area : Left atrium
- Influenced by: 受很多因素影响
- Hypotension 低血压
- Acute MR - underestimate
急性二尖瓣反流 - 低估 - Eccentric jet - underestimate
偏心性反流 - 低估 - Colour gain
色彩增益 - Nyquist limit
尼奎斯特极限
| Mild | Moderate | Severe |
|---|---|---|
| < 20% | 20% - 40% | > 40% |
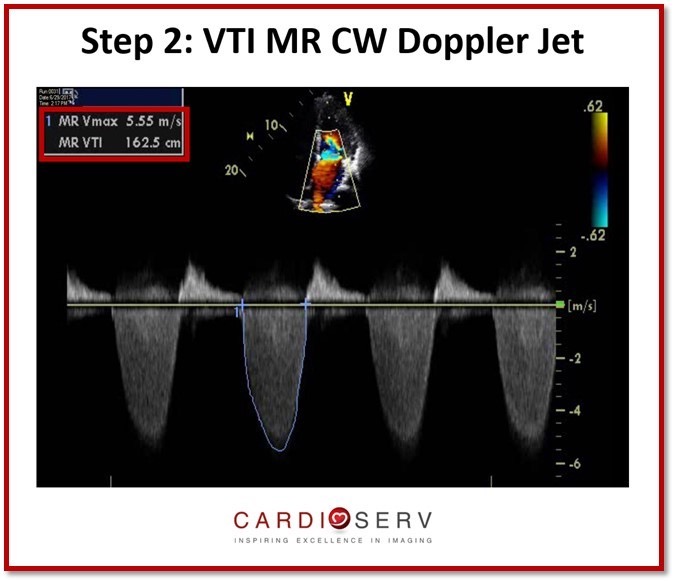
# Continuous Wave at MR jet 反流束连续波多普勒
- Assessed in A4C or A2C
在心尖四腔心或心尖两腔心评估 - CW at MR jet
在二尖瓣反流束上放置连续波多普勒 - Qualitative approach
定性方法 - Difficult to obtain if eccentric jet.
如果是偏心性反流,则很难获得
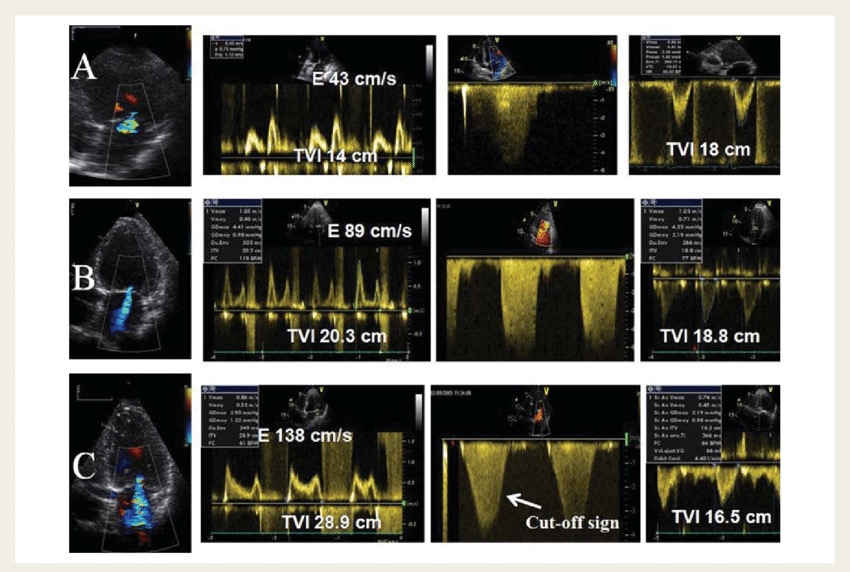
- Three examples of various degrees of mitral regurgitation (MR), mild (A), moderate (B), and severe (C) are provided.
三个不同程度的二尖瓣返流 (MR) 的例子:轻度 (A)、中度 (B) 和重度 (C)。 - The regurgitant jet as well as the mitral E wave velocity increase with the severity of MR.
二尖瓣反流及二尖瓣 E 峰速度随 MR 严重程度的增加而增大。 - In severe MR, the continuous wave Doppler signal of the regurgitant jet is truncated, triangular and intense.
在重度 MR 时,反流的连续波多普勒信号被截断,呈三角形且信号灰度较强。 - Notching of the continuous wave envelope (cut-off sign) can occur in severe MR.
重度 MR 中可能会发生连续波轮廓的缺口 (切断征象)。 - TVI, time-velocity integral. 时间 - 速度积分
| Mild | Severe |
|---|---|
|
|
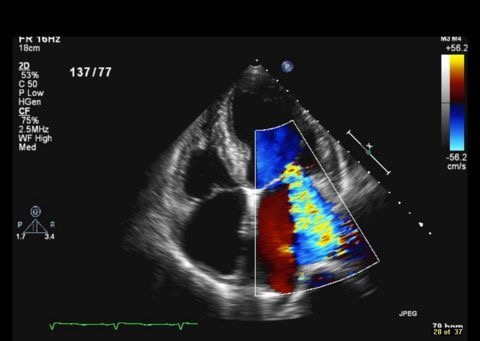
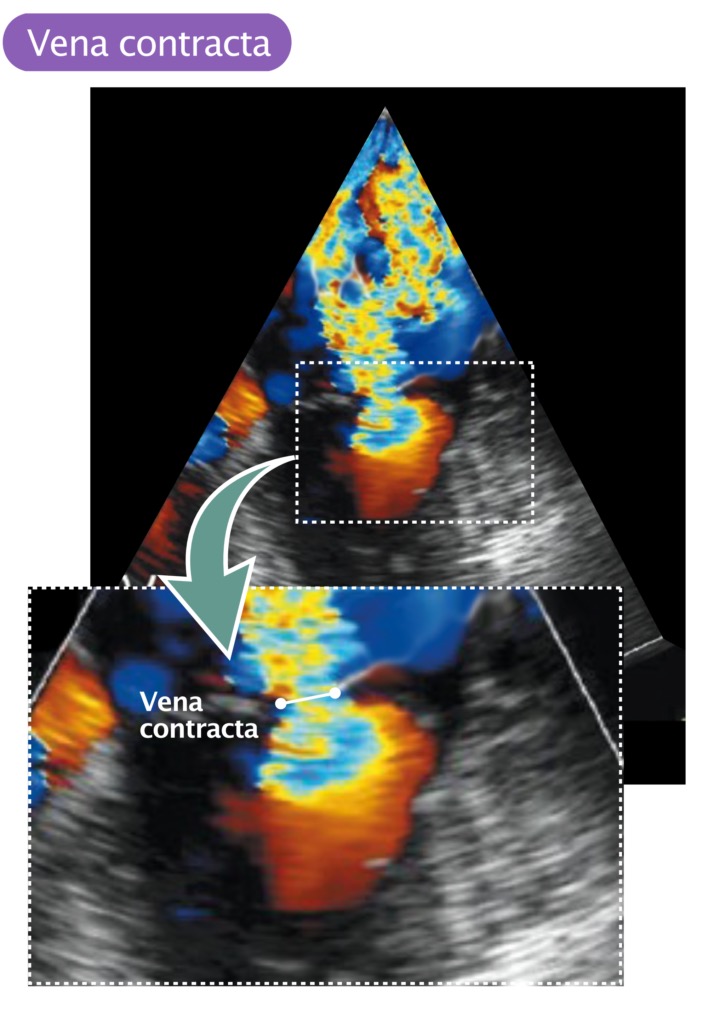
# Vena Contracta 缩流颈
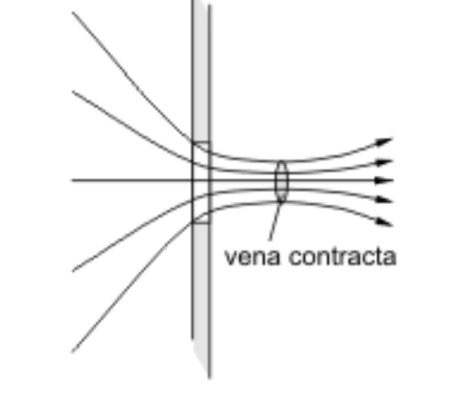
, VC, and jet area.")
- PLAX or A4C
胸骨旁长轴 或 心尖四腔心切面- Remember: A2C is not recommended for this technique as it over estimates VC.
记住:心尖两腔心切面不推荐用于 VC 测量,因为会导致结果高估
- Remember: A2C is not recommended for this technique as it over estimates VC.
- Zoom in on mitral valve
放大二尖瓣 - CFM at mitral valve
在二尖瓣加持彩色多普勒 - Nyquist limit 50-60cm/s
尼奎斯特极限 - Measure narrowest portion of jet as it emerges from the orifice
当反流束从反流口喷射出来时,测量反流束最窄的部分 - More accurate for central MR
对于中心性 MR 更准确,偏心性反流有时不太容易看到 - Can be used in multiple jets
可用于多束反流- 缩流颈宽度 VCW = 低估,不能相加(3D 计算横截面积 VCA 可相加)
| Mild | Severe | |
|---|---|---|
| < 3mm | If intermediate then need another technique to quantify MR | ≥ 7mm |
# Pulmonary Veins 肺静脉
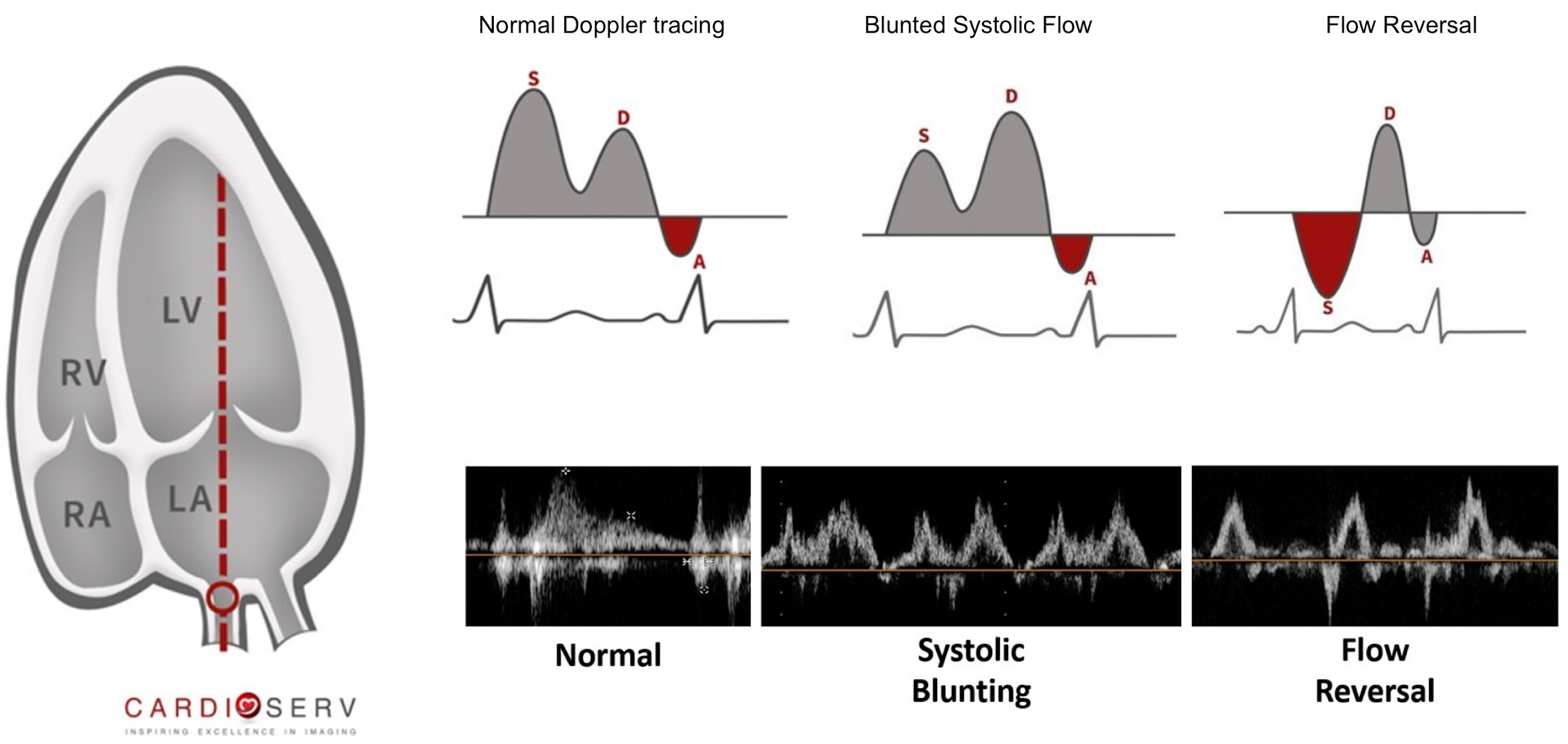
- Apical 4 chamber
心尖四腔心 - CW at pulmonary vein
在肺静脉放置连续波多普勒 - Influenced by LA pressure and diastolic function
受左房压力和舒张功能的影响 - Not accurate in atrial fibrillation
房颤时不准确
| Normal | Severe |
|---|---|
S (systolic wave) > D (diastolic wave) | Retrograde flow during ventricular systole |
# Mitral Inflow Pattern 二尖瓣血流频谱
- Apical 4 chamber
心尖四腔心测量 - Pulsed wave doppler at MV annulus
在二尖瓣瓣环处放置脉冲波多普勒 - Affected by LA pressure and diastolic function
受左房压力和舒张功能的影响 - Not accurate in AF
房颤时不准确

- (A) Pulsed Doppler of normal mitral inflow characteristically shows an early diastolic E-wave followed by the atrial A wave.
正常二尖瓣血流的脉冲多普勒表现为舒张期早期 E 波,然后是房性 A 波。 - (B) In severe mitral regurgitation (MR), marked E-wave dominance is seen (>1.2 m/s), reflecting a marked increased in early diastolic flow—typical of severe MR.
在重度二尖瓣反流中,可见明显的 E 波优势 (>1.2m/s),反映早期舒张期血流明显增加 -- 这是重度 MR 的典型表现。
| Excludes severe MR | Severe MR |
|---|---|
A wave dominant |
|
# Quantitative methods 定量方法
- Effective Regurgitant Orifice Area (EROA)
有效反流口面积(EROA) - Regurgitant Volume
反流容积 - Regurgitant Fraction
反流分数 - Can be assessed using:
可以使用以下方法进行评估:- PISA / flow convergence or doppler volumetric method
近端等速表面积 / 血流收敛方法或多普勒容积法
- PISA / flow convergence or doppler volumetric method
- These methods can help in intermediate MR patients
这些方法可以诊断中度 MR 患者
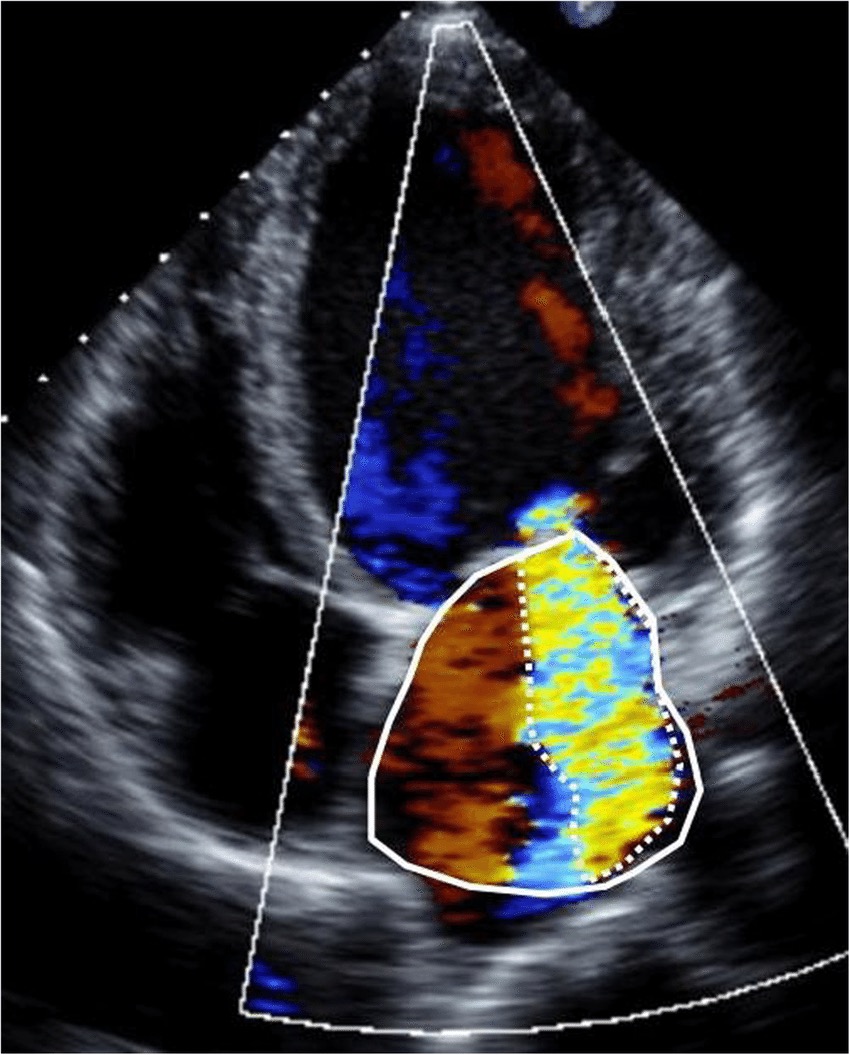
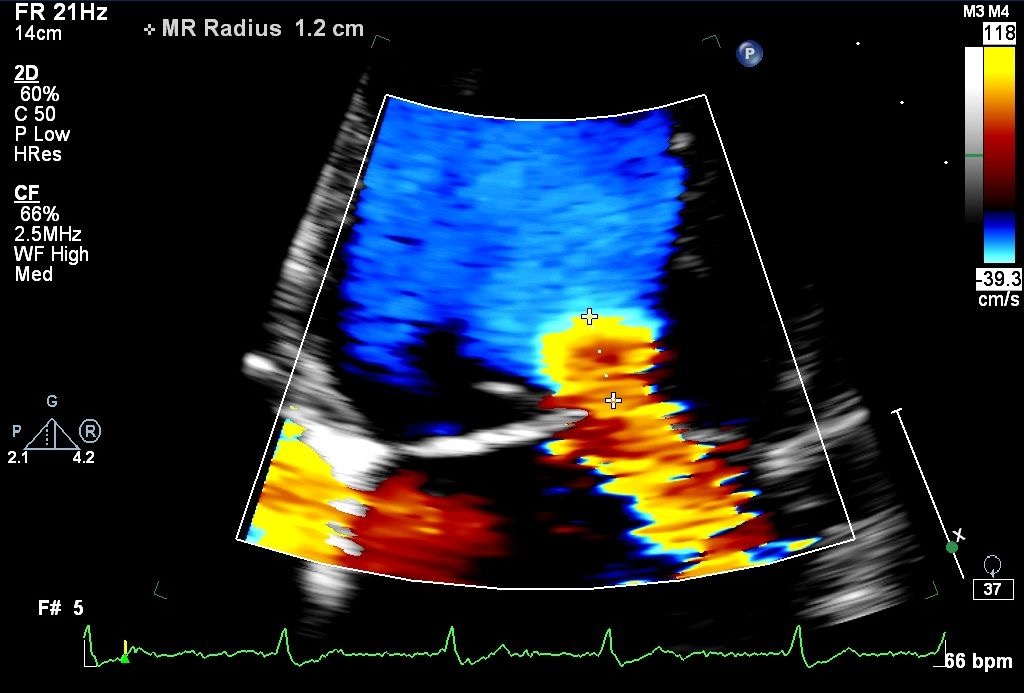
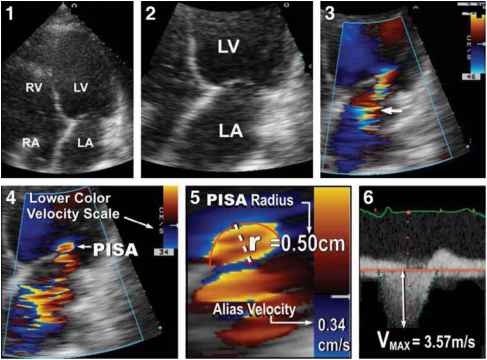
# PISA Method
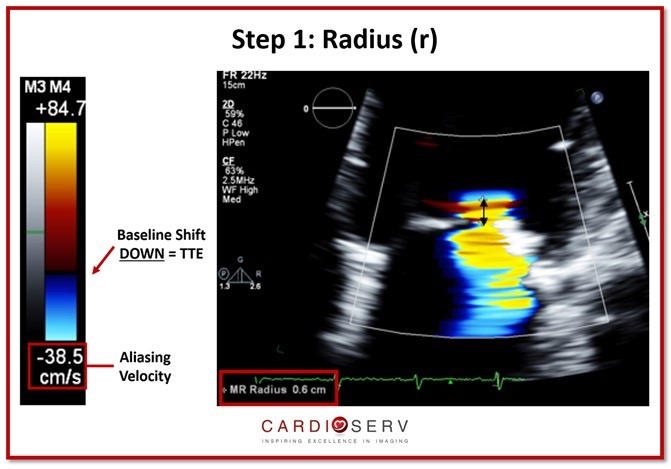
# Proximal Isovelocity Surface Area (PISA) Radius 近端等速表面积 (PISA) 半径
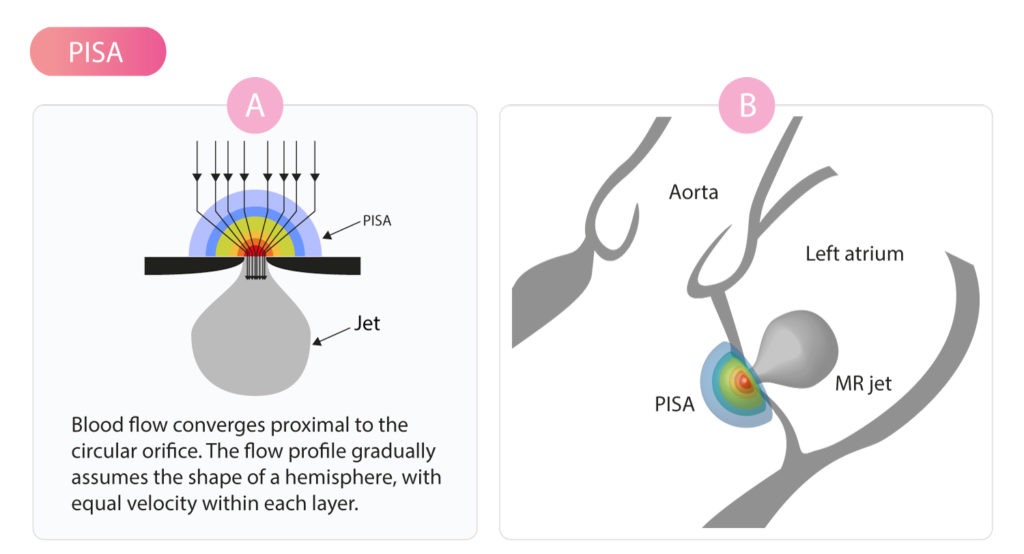
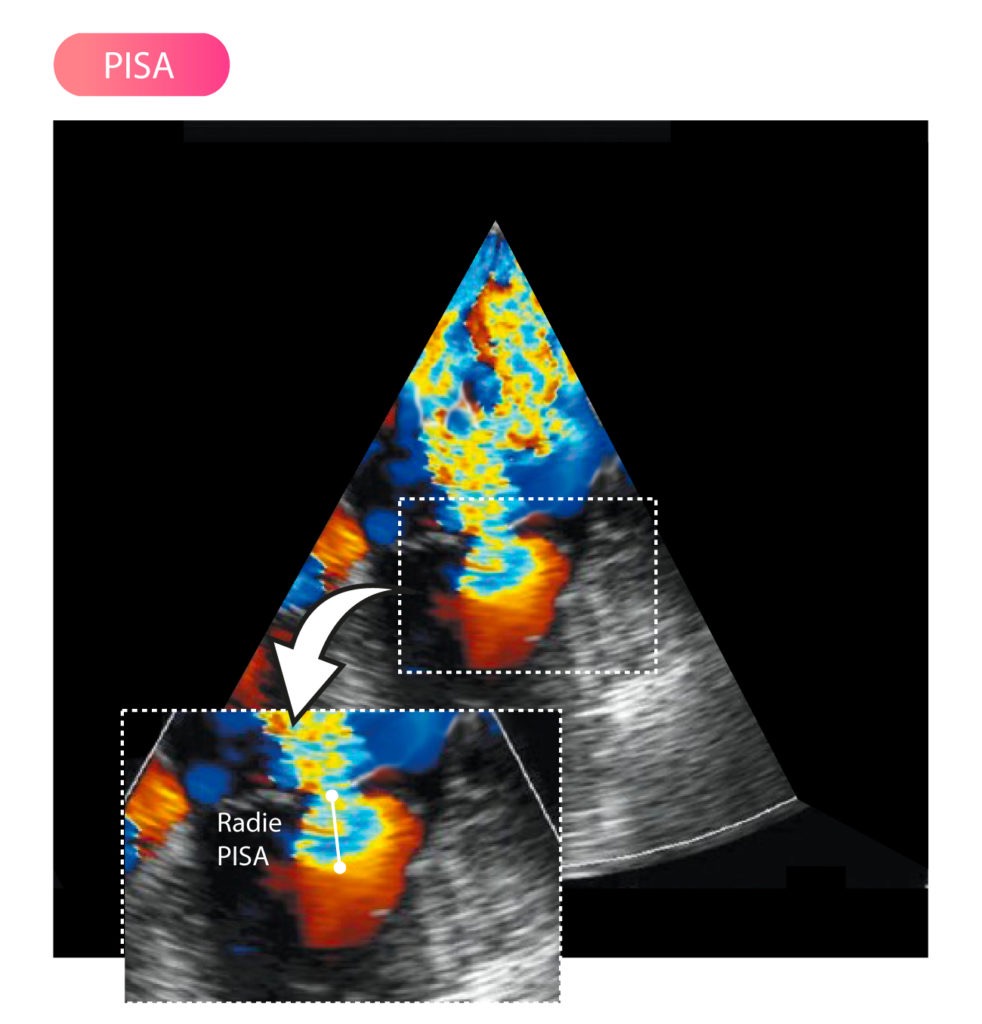
PISA 是液体流过圆形孔口时发生的一种现象。血流在开口附近收敛并加速 (Flow Convergence),血流剖面逐渐形成多层的半球形状,每层内的流速相等。
PISA 位于反流口近端,本身是半球形,在 2D 下看显示为半圆形,其半径是从颜色混杂的边缘到缩流颈的距离。
Measure from the vena contracta to first aliasing threshold
测量从缩流颈到第一个混叠阈值的距离Apical 4 chamber
心尖四腔心Zoom at MV leaflets
放大二尖瓣瓣叶Baseline to 30-40cm/s
彩色速度基线需朝反流方向调整至 30-40 cm/s- TTE:朝下;TEE:朝上
| Mild | Moderate | Severe |
|---|---|---|
| < 0.4cm | 0.4 - 1.0cm | > 1.0cm |
# Effective Regurgitant Orifice Area 有效反流口面积
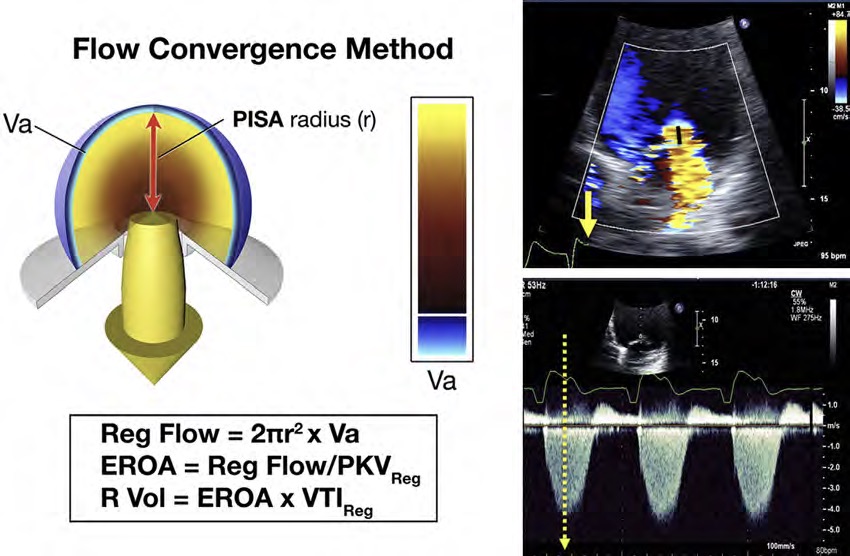
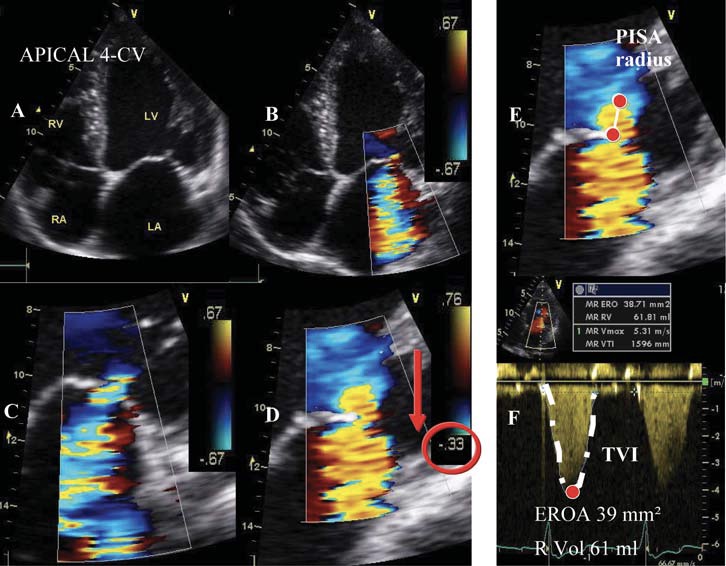
- PISA Equations
| Mild | Moderate | Severe |
|---|---|---|
| < 0.2 cm2 | 0.2 - 0.39 cm2 | ≥ 0.40 cm2 |
 (hemielliptic) and organic mitral regurgitation (B) (hemispheric).")
- Flow convergence pattern differs depending on the aetiology of MR
因 MR 病因不同,血流会聚模式存在不同- Functional MR (hemielliptic)
功能性 MR(呈半椭圆形) - Organic MR (hemispheric)
器质性 MR(呈半球形)
- Functional MR (hemielliptic)
- European guidelines have a different cut off for EROA to account for this:
欧洲指南对 EROA 的参考范围有所不同- Severe functional MR ≥ 20 mm2
- Severe primary MR ≥ 40 mm2
# Regurgitant Volume 反流容积
| Mild | Moderate | Severe |
|---|---|---|
| < 30ml | 31-59ml | ≥ 60ml |
# Limitations to PISA Method 方法的局限性
- Assumes the EROA is constant throughout systole
假设 EROA 在整个收缩期间是恒定的 - Assumes EROA is hemispheric in shape
假设 EROA 为半球形 - PISA method more accurate for organic MR
PISA 法对器质性病变更准确- Rheumatic MR - Constant PISA radius
风湿性二尖瓣反流 - PISA 半径恒定 - Mitral valve prolapse - PISA radius increases progressively and peaks around mid-systole
二尖瓣脱垂 - PISA 半径逐渐增大并在收缩中期达到峰值 - Functional MR - Early systolic peak with mid systolic decrease and late systolic peak (bimodal)
功能性 MR - 收缩早期即达到峰值,收缩中期下降,收缩晚期再次达到峰值 (双峰)
- Rheumatic MR - Constant PISA radius
# Volumetric Method 容积法
# Continuity equation 连续方程式
Assumes that there is no significant AR.
假设不存在严重的主动脉瓣反流每搏量计算
If there is no MR,
Regurgitant Volume 反流容积计算
| Mild | Severe |
|---|---|
| < 30ml | ≥ 60ml |
- Regurgitant Fraction 反流分数计算
| Mild | Moderate | Severe |
|---|---|---|
| < 30% | 31-49% | ≥ 50% |
- EROA 有效反流口面积
| Mild | Moderate | Severe |
|---|---|---|
| < 0.2cm2 | 0.2 - 0.39cm2 | ≥ 0.40cm2 |
# Example
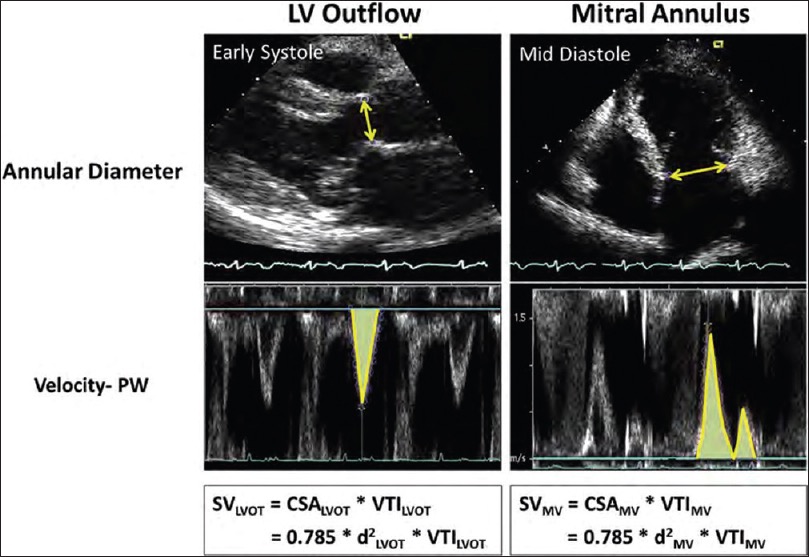
Echo-Doppler calculations of stroke volume at the left ventricular outflow tract and mitral valve annulus sites.
左心室流出道和二尖瓣环处每搏量的超声多普勒计算。
左室长轴,收缩早期,LVOT 测径线,并放置 PW 描绘频谱获得 LVOT VTI。
四腔心,舒张中期,测二尖瓣瓣环直径 + 在测量径线的位置放置 PW 描绘 二尖瓣 E 峰和 A 峰获得 VTIIn this example of severe mitral regurgitation, SVMV was 183 mL (d = 3.5 cm, velocity time integral =19 cm) and SVLVOT was 58 mL (d = 2.3 cm, velocity time integral =14 cm).
在这个严重二尖瓣反流的例子中,SVMV 为 183ml(d=3.5cm,速度时间积分 = 19cm),SVLVOT 为 58ml(d=2.3cm,速度时间积分 = 14cm)。This yielded an regurgitant volume of 125 mL and a regurgitant fraction of 125/183 or 68%.
这产生了 125 mL 的反流容量和 125/183 或 68% 的反流分数。d: Diameter of the annulus, PW: Pulsed wave Doppler
D:瓣环直径,PW:脉冲多谱勒
# Limitation
- Time-consuming 耗时
- PISA is first line method in quantifying MR
PISA 是量化 MR 的一线方法 - Potential errors due to multiple measurements
推导过程中的多次测量可能导致潜在误差 - Accurate resolution of the MV annulus is needed
需要对 MV 瓣环进行准确的分辨
# Left Ventricle
Compensated phase: 代偿阶段
Stroke volume is maintained through an increase in LV EF (hyperdynamic LV> 65%)
通过增加 LV EF (高动力左室> 65% ) 来维持每搏量Decompensated phase: 失代偿阶段
Stroke volume decreases and LA pressure increases - LV function may be low normal range
每搏量减少,左房压力升高 —— LV 功能可能正常偏低

# Left Atrium
- LA dilates in response to chronic volume and pressure overload
左房扩张是对慢性容量和压力超负荷的反应 - Normal sized LA not associated with significant MR, unless it is acute
正常大小的 LA 与严重 MR 无关,除非 MR 是急性的 - LA dilatation predicts increased risk of AF
左房扩张预示房颤风险增加 - MV repair or replacement leads to reverse remodelling of the LA
MV 修复或置换可使 LA 逆重塑

- Left Atrial Volume
- A significantly dilated left atrium is a predictor for worse outcomes in organic severe MR.
左心房明显扩张是器质性重度 MR 预后较差的预测指标。
| Normal | Mild | Moderate | Severe |
|---|---|---|---|
| 16-28ml | 29-33ml | 34-39ml | ≥ 40ml |
# Pulmonary Artery Systolic Pressures 肺动脉收缩压
Excess mitral regurgitant flow entering the LA causes increase LA pressure
进入左房的二尖瓣返流过多导致左房压力升高This results in a raised pulmonary pressure
这导致肺动脉压升高TR max gradient + RAP (IVC size and collapsibility) to estimate pulmonary pressures.
TR 最大压差 + RAP(下腔静脉大小和收缩性)以估计肺压力。PASP > 50mmHg at rest is an indication for MV repair
静息时 PASP >50 mmHg 是 MV 修复的指征
# Special tests in MR 其他特殊手段
# Exercise Echocardiography 运动负荷超声心动图
- Useful in asymptomatic patient with severe organic MR and borderline EF (60-65%)
适用于无症状的严重原发性 MR 伴临界 EF(60-65%)的患者 - If there is an absence of contractile reserve it could identify patients at risk of cardiovascular events
如果没有很好的收缩储备,可认为患者有较高的心血管事件风险 - Equivocal symptoms out of proportion of MR severity
可疑症状与 MR 严重程度不成比例时用作参考- PASP > 60mmHg on exercise is an indication for Mv repair.
运动时 PASP > 60 mmHg 为 MV 修复的指征
- PASP > 60mmHg on exercise is an indication for Mv repair.
# 3D Echocardiography
- Provides improved definition of mitral morphology
改善了二尖瓣形态的显示

# Summary
- The main methods (anatomical, semi-quantitative and quantitative) for assessment of mitral regurgitation
评估二尖瓣反流的主要方法(解剖学、半定量和定量) - The advantages and limitations of each of these methods
每种方法的优点和局限性 - The need to integrate information from each of these to reach a final assessment of mitral regurgitation severity
需要综合这些信息以得出二尖瓣反流严重程度的最终评估 - A brief discussion of more advanced techniques
简要讨论了更先进的技术。