# Learning objectives
- To understand the epidemiology, aetiology, pathophysiology and prognosis of aortic regurgitation
了解主动脉瓣反流的流行病学、病因学、病理生理学及预后 - To review the qualitative and quantitative echocardiographic methods available to assess severity
回顾可用于评估严重程度的定性和定量超声心动图方法 - To appreciate the role of echocardiography in the management of aortic regurgitation.
了解超声心动图在主动脉瓣反流治疗中的作用
# Aetiology 病因
# Leaflet (Disease of valvular apparatus) 瓣叶 (瓣膜疾病)
- Rheumatic - Leading cause in non-Western countries
风湿性瓣膜病 - 在非西方国家的主要病因 - Myxomatous 粘液瘤
- Calcific degenerative 钙化退行性变
- Endocarditis 心内膜炎
- Connective tissue disorders (SLE and Rheumatoid arthritis)
结缔组织病 (系统性红斑狼疮和类风湿关节炎) - Trauma 创伤
- VSD - Supracristal associated with cusp prolapse.
室间隔缺损 - 与瓣尖脱垂相关的脊上室间隔缺损。
缺损(箭头)位置靠近主动脉瓣,是导致主动脉瓣关闭不全的常见原因。血液从左向右分流通过缺损被认为通过 Venturi 效应逐渐拉动主动脉瓣组织(尤其是右冠瓣尖)导致脱垂样改变(***)![]()

# Root Disease 根部病变
- Hypertension 高血压
- Dissection
- Connective tissue disorders, such as Marfan syndrome and Ehlers Danlos
结缔组织疾病,如马凡综合征和埃勒斯・丹洛斯 - Syphilitic 梅毒
- Sinus of Valsalva aneurysm
瓦氏窦瘤
# Combination of valve and root 两者均有
- Bicuspid valve disease
二叶式 - Ankylosing spondylitis
强直性脊柱炎
# Pathophysiology and Haemodynamics
# Acute Aortic Regurgitation
# Aetiology
- Infective endocarditis 感染性心内膜炎
- Aortic dissection 主动脉夹层
- Trauma 创伤
# Medical emergency
- Untreated LVEDP rises rapidly
未经治疗的左室舒张末压急速上升 - Increasing heart rate and contractility to cope with the regurgitant volume (preload).
心率和收缩能力增加以应对反流量 (前负荷)。 - Effective stroke volume cannot be maintained despite compensatory mechanisms
尽管有代偿机制,仍不能保持有效的每搏量 - Rapid pulmonary oedema, cardiogenic shock and death.
急性肺水肿、心源性休克和死亡
# Chronic Aortic Regurgitation
- Chronic AR, however, allows the LV to adapt and remodel, delaying the onset of symptoms.
慢性 AR 允许左室适应和重塑,延迟症状的出现。 - A summary of the changes include(Echo features in italics.):
改变包括(超声表现用斜体标识):Left ventricular volume and pressure overload
左心容量和压力负荷增加Increase in LV wall stress
左室壁应力增加Compensatory hypertrophy (concentric and eccentric) in an attempt to normalise wall stress
代偿性肥厚 (向心性和偏心性) 试图使室壁应力正常化Systolic hypertension (often) as a consequence of increased stroke volume
由于每搏量增加而引起的 (通常) 收缩期高血压Pulse pressure widening as aortic diastolic blood pressure drops due to regurgitation back into the LV
由于反流回到左室,主动脉舒张压下降,脉压变宽During initial stages, the regurgitant volume increases LVEDV without an increase in LVEDP as the LV dilates and compliance increases
在初始阶段,随着左室扩张和顺应性增加,反流容积使左室舒张末容积增加,但不会增加左室舒张末压力Despite the compensatory mechanisms, however, LVEDP eventually rises as systolic dysfunction supervenes
尽管有代偿机制,随着收缩功能障碍的产生,左室舒张末压力最终还是会升高Late onset of symptoms - The end-stage heart often resembles a spherical, dilated LV with increased mass and is so called cor a bovinum (bovine or ox heart).
晚期症状 - 终末期心脏通常类似球形,左室全扩张,质量增加,EF 低,被称为牛心。此时再手术已经晚了
# Severe Chronic Aortic Regurgitation 重度慢性反流
- Rising LV Diastolic pressures:
左室舒张压升高,导致:- Quieter/shorter early diastolic murmur
舒张早期杂音更安静、更短 - Early mitral closure
二尖瓣关闭提前 - Diastolic mitral closure
舒张期二尖瓣关闭 - Steeper diastolic slope.
陡峭的舒张期斜率
- Quieter/shorter early diastolic murmur
- Timing of surgery critical:
关键手术时机:- Survival is reduced if
随着以下情况的出现,生存率降低- LVESD > 50mm
- EF < 50%
- Symptoms especially of heart failure.
尤其是心力衰竭的症状
- Survival is reduced if
# 2D echo
# Valve leaflet clues 瓣叶线索
Congenital abnormalities 先天性异常
- Is the valve tricuspid? 是三叶式吗
- Is there evidence of eccentric coaptation? (Unicuspid, bicuspid, quadricuspid).
对合点是否不居中,胸骨旁长轴看对合点呈偏心状态 (单叶式、二叶式、四叶式)。
Acquired abnormalities 获得性异常
- Is there cusp thickening, calcification?
有无瓣叶增厚或钙化? - Are other valves affected? (Rheumatic)
其他瓣膜是否有影响?(风湿性) - Is there evidence of perforation or vegetations? (Endocarditis)
有无穿孔或赘生物的证据?(心内膜炎) - Are the cusps thickened with redundant leaflets?
有无瓣叶冗余? - Is there diastolic sagging into the LVOT? (Myxomatous)
有无左室流出道舒张期下垂?(粘液瘤) - Is leaflet motion restricted? (Co-existent aortic stenosis)
瓣叶运动是否受限?(合并主动脉瓣狭窄) - Is there leaflet prolapse? (False channel secondary to aortic dissection)
有无瓣叶脱垂?(主动脉夹层继发的假腔)
- Is there cusp thickening, calcification?
# Root clues 根部线索
Aortic Root 主动脉根部
- Is there dilation with maintenance of normal contours and narrowing at the sinotubular junction? (degenerative disease)
窦管交界是否扩张,是否保持正常轮廓和狭窄?(退行性疾病)
- Is there dilation with maintenance of normal contours and narrowing at the sinotubular junction? (degenerative disease)
Is there effacement? 窦管交界是否消失
- ie. enlargement of the sinuses of Valsalva accompanied by loss of narrowing at the sino-tubular junction? (Marfan syndrome)
瓦氏窦增大,并伴有窦管交界处的狭窄消失?(马凡综合征)
- ie. enlargement of the sinuses of Valsalva accompanied by loss of narrowing at the sino-tubular junction? (Marfan syndrome)
Is the aortic root extensively calcified?
主动脉根部是否广泛钙化?- Syphilis 梅毒
Is there evidence of a false channel/dissection flap?
是否有假腔 / 夹层皮瓣的证据?- Aortic dissection 主动脉夹层
# Indirect clues
# The left ventricle
Hypertrophy 肥大
- Is there concentric hypertrophy i.e. increased LV mass and relative wall thickness?
是否有向心性肥厚,即左心室质量和相对室壁厚度增加 - Typically seen with isolated hypertension and pressure overload
典型表现为孤立性高血压和压力超负荷 - Is there eccentric hypertrophy? i.e. increased LV mass but normal relative wall thickness? (Typically as a consequence of volume overload).
是否有偏心肥大?LV 质量增加,但相对壁厚正常?(通常是由于体积过载)
- Is there concentric hypertrophy i.e. increased LV mass and relative wall thickness?
Size 大小
- Is the LV dilated? 是否有扩张
- Suggestive of chronicity of AR and increasing severity.
提示 AR 慢性加重
Function 功能
- Is LV function diminished? 左室功能是否减弱
- This implies haemodynamically severe AR although alternative causes of impaired function should be borne in mind.
意味着血液动力学上严重的 AR,尽管应考虑其他导致功能受损的原因。
Relative wall thickness 相对壁厚
- In the presence of increased LV mass, RWT greater than 0.42 indicates concentric hypertrophy. RWT less than 0.42 defines eccentric hypertrophy.
当左室重量增加时,RWT 大于 0.42 表示向心性肥厚。RWT 小于 0.42 定义为偏心性肥厚。






,主动脉根部扩张 (窦管交界的狭窄无消失),对合点还是居中的,形态保留")
 Marfan syndrome,主动脉根部扩张(窦管交界/形态消失),马凡综合征")

# Doppler Assessment 多普勒评估
# Qualitative 定性
# Jet area/length in LV cavity 左室腔内的反流束面积或长度
不是非常精确,因为技术和机器的参数设置会影响到成像
- In apical views, measure how far the regurgitation extends into the LV cavity using colour and Pw Doppler.
心尖切面中,使用彩色多普勒和 PW 测量反流延伸到 LV 腔的程度。 - Regurgitation reaching the end of the anterior mitral valve leaflet is indicative of moderate severity.
反流到达二尖瓣前叶末端提示中度 - Jets extending beyond and into the body of the LV indicate severe disease.
反流束射出并进入左室腔内提示重度 - Set a Nyquist limit (aliasing velocity 50-60 cm/sec) and optimise colour gain such that randlom colour speckle from non-moving regions is just eliminated.
设置 Nyquist 极限(混叠速度 50-60 厘米 / 秒),并优化色彩增益,从而消除来自静止区域的随机色彩斑点
- Limitations of colour flow mapping 彩色多普勒的局限性
- Colour Doppler is heavily dependent on Pulse Repetition Frequency (PRF) and colour gain.
彩色多普勒在很大程度上取决于脉冲重复频率 (PRF) 和彩色增益。- Jet area includes both turbulent (aliased) and laminar flow, which may result in overestimation of central jets.
射流区域包括湍流 (混叠) 和层流,这可能会导致对中心射流的高估。- Increasing the scale may underestimate jet area.
增大范围可能会低估反流束面积。- The length of the regurgitant jet is similarly influenced by the above factors.
反流射流束的长度也同样受上述因素的影响。
# CW Doppler AR jet density
- The intensity of the regurgitant signal seen on CW spectral display in apical 3-or 5-chamber views reflects the volume of regurgitation compared to forward flow through the aortic valve.
心尖 3 腔或 5 腔切面下,CW 反流频谱图的灰度,通过主动脉瓣的前向血流相比,信号强度反映了反流容积。 - While a weak regurgitant signal compared to forward flow is consistent with minimal AR, greater degrees of regurgitation produce equal density of retrograde and antegrade flow signals.
虽然与前向血流相比,反流信号较弱,与最小 AR 相一致,但反流程度越大,逆行和顺行血流信号密度越相近。灰度与前向血流越相似,斜率下降越快越陡峭,提示严重程度高 - Reliable discrimination between moderate and severe grades of regurgitation, however, is not possible based on signal intensity alone.
然而,仅凭信号强度(灰度)受很多设置影响,是不可能可靠的区分中度和重度反流的。
# Semi-Quantitative 半定量
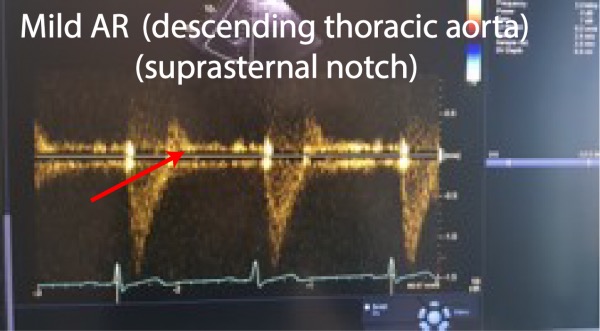
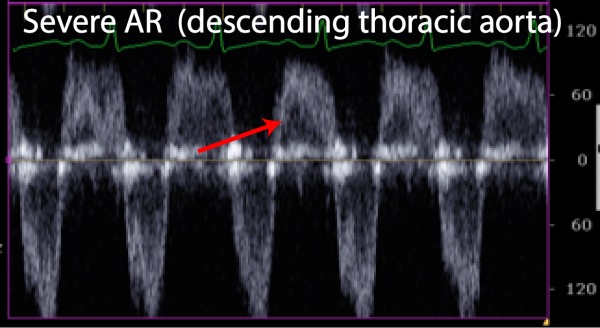
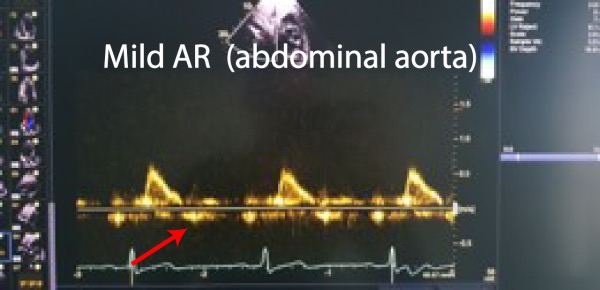
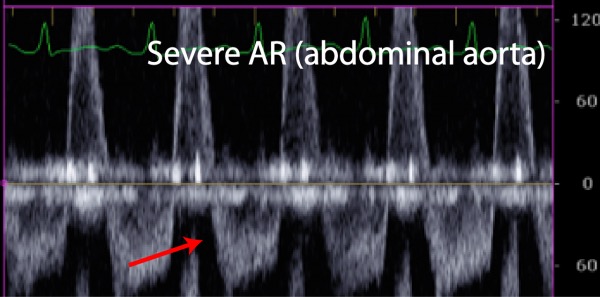
# Diastolic flow reversal - Descending Aorta 舒张期血流逆转 - 降主动脉

Using a suprasternal view, PW Doppler interrogation of the upper descending aorta may detect brief (early) reversal of diastolic aortic flow even in normal individuals.
即使在正常人中,使用胸骨上切面,PW 检测降主动脉上部也可以检测到舒张期主动脉血流的短暂(早期)逆转。As regurgitation becomes more severe, flow reversal occupies a greater period of diastole. Thus, diastolic flow velocities increase.
随着反流变得更加严重,血流逆转占据了更大的舒张期(反向血流的持续时间)。因此,舒张期血流速度增加(反向血流的速度)。Descending thoracic aortic holo-diastolic flow reversal indicates, at least, moderate AR.
降主动脉全舒张期血流反转至少为中度 AR。Limitations - Varying degrees of flow reversal may also be seen with age-related changes in rigidity and diminishing compliance of the aortic wall.
局限性 - 随着年龄的增长,主动脉壁的硬度和顺应性降低,也可以看到不同程度的血流逆转。
# Quantitative 定量
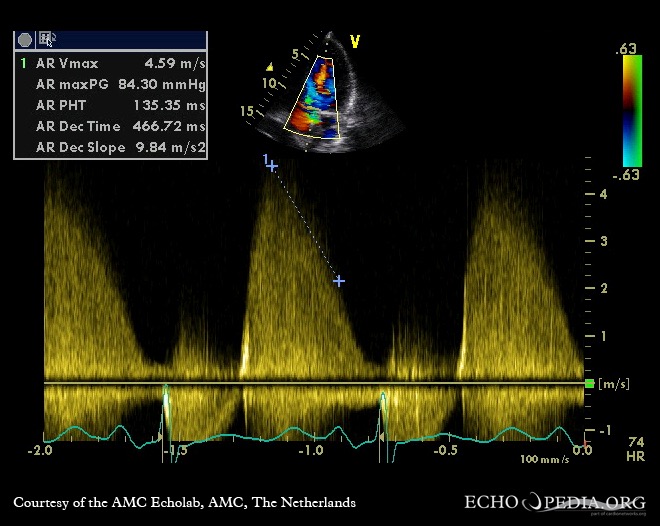
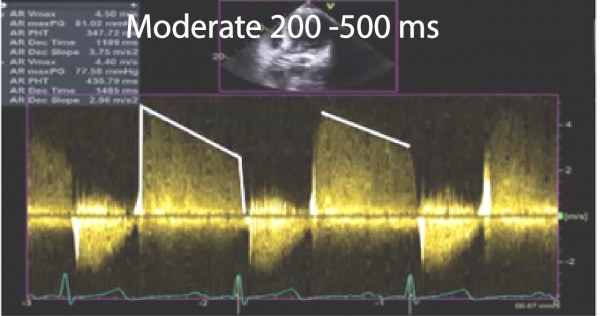
# Pressure half-time and jet deceleration rate 压力减半时间和反流减速率

- Use Apical 5- or 3-chamber views
心尖五腔或三腔心切面 - Align CW Doppler (aidled by colour flow mapping) along the direction of the jet
沿反流方向对齐连续波多普勒 (通过彩色多普勒) - Measure peak velocity and the slope of the flat part of the spectral trace, i.e. deceleration slope, hence, pressure half-time
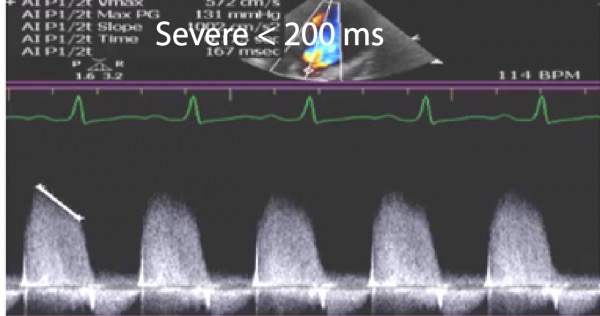
测量频谱平坦部分的峰值速度和斜率,即减速斜率,即压力半衰期 - As severity of regurgitation increases
随着反流严重程度的增加- Aortic diastolic pressure falls more rapidly
主动脉舒张压下降更快 - Late-diastolic velocity is lower / deceleration slope steeper
舒张晚期血流速度较低 / 减速斜率较陡 - Short pressure half-time.
压力减半时间短暂
- Aortic diastolic pressure falls more rapidly
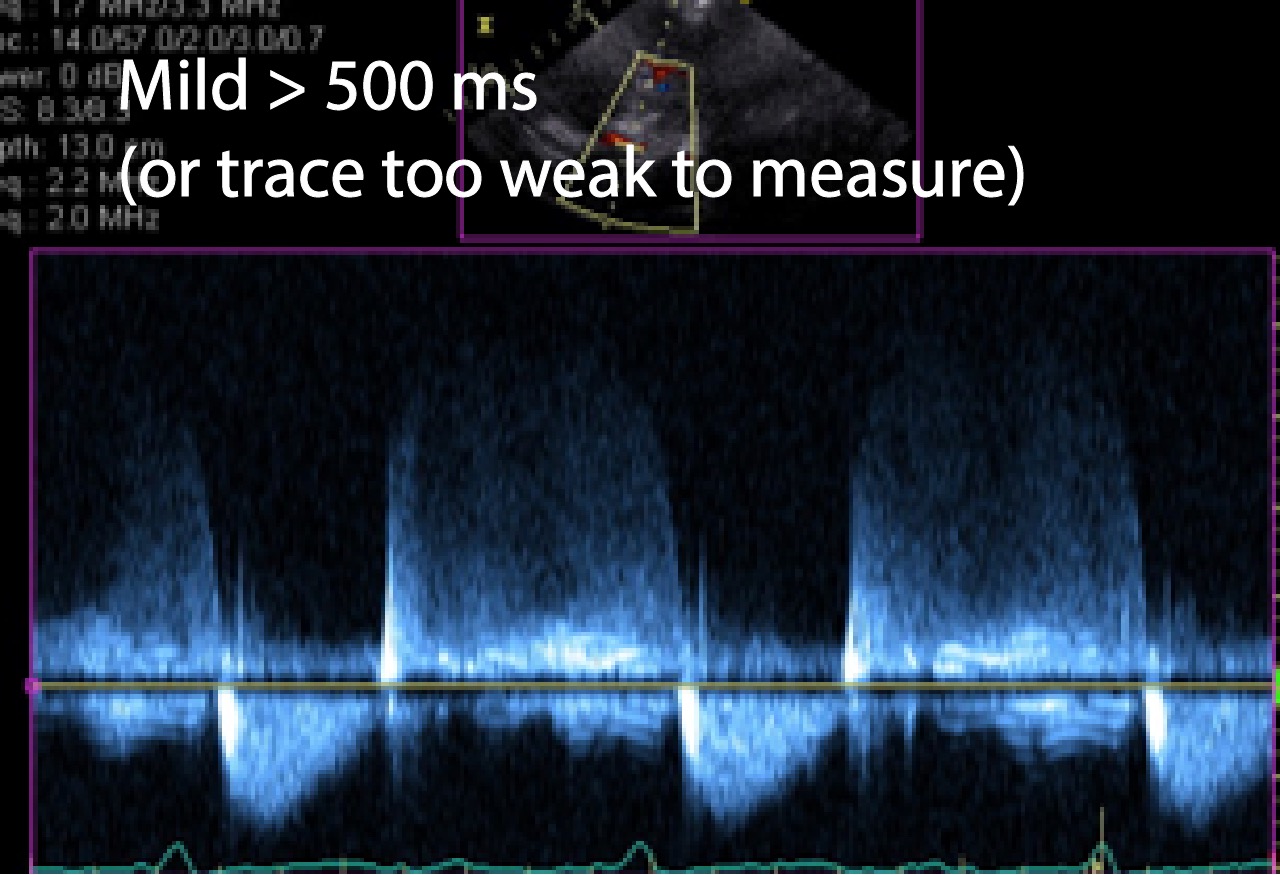
Valve Regurgitation Pressure half-time
瓣膜反流压力半时间- Relevant to AR and PR
- Again, the more severe the AR, the STEEPER the slope (i.e. the more severe the regurgitation the earlier the pressure equalizes and flow reduces/stops).
同样,AR 越严重,斜率越陡峭 (即,反流越严重,压力越早均衡并且流量减少 / 停止)。
Limitations of Pressure Half-time 局限性
- The PHT with be affected by:
- LV compliance especially in chronic AR
左室顺应性,尤其是慢性 AR 患者 - LV diastolic pressure (e.g. systolic dysfunction, ischaemia) and
左室舒张压 (如收缩功能障碍、缺血) 和 - Aortic diastolic pressure (e.g. sepsis, patent ductus arteriosus, vasodilators)
主动脉舒张压 (如败血症、动脉导管未闭、血管扩张剂) - With chronic AR, LV function and aortic compliance change to accommodate the larger regurgitant volumes, slowing down the equalisation of trans-aortic pressures and lead to misleadingly longer pressure half-time values and underestimation of AR.
慢性 AR、LV 功能和主动脉顺应性发生变化以适应更大的反流量,减慢经主动脉压力的平衡,并导致误导性的较长的压力减半时间,导致低估 AR 的程度。
- LV compliance especially in chronic AR
- Hence: 因此
- More useful as a marker of severity in acute regurgitation
作为急性反流严重程度的标志更有用 - Since LV compliance will not have adapted so quickly.
因为 LV 顺应性不会如此迅速地适应。
- More useful as a marker of severity in acute regurgitation
- The PHT with be affected by:
# Vena Contracta
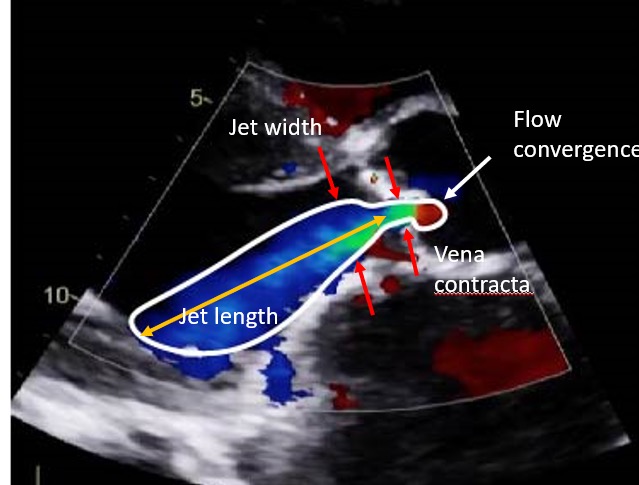
Vena Contracta VC width is the narrowest portion of colour flow at or just below the level of the aortic valve.
缩流颈宽度是在主动脉瓣水平或正下方的彩色血流的最窄部分。Calculation: Measure in parasternal windows since better axial resolution is offered compared to apical windows. Use zoom and colour M-mode to minimise errors in measurement.
测量方式:在胸骨旁视窗测量,因为与心尖视窗相比,能提供更好的轴向分辨率。使用局部放大和彩色 M 模式将测量误差降至最低。Limitations: VC width is not reliable with: 局限性
- Multiple jets 多个反流束
- Irregularly shaped jet 不规则的反流束
- Care with eccentric jets - Measurements must be made perpendicular to the direction of the jet rather than to the long axis of the LVOT
注意偏心射流 - 测量必须垂直于反流束方向而不是垂直于 LVOT 的长轴 - Relatively small values of VC width (usually < 1cm) leads to potentially large measurement errors.
VCW 相对较小(通常<1cm)会导致潜在的较大测量误差。
# Jet width / LVOT width 反流束与左室流出道宽度之比
- The regurgitant jet width to LVOT diameter ratio refers to the maximal proximal jet width measured in the LVOT.
反流束宽度与左室流出道直径之比是指在 LVOT 中测得的最大近端反流束宽度。 - Calculation: Similar to VC width measurements, use parasternal windows with zoom and/or colour M-mode to maximise axial and temporal resolution.
与 VC 宽度测量类似,使用局部放大和 / 或彩色 M 模式的胸骨旁视窗来最大化轴向和时间分辨率。 - Limitations: 局限性
- Unpredictably expansion below the valve orifice potential source of error
瓣膜下方不可预测的膨胀可能是误差的根源 - Measurement too far below the valve tends to overestimate severity as the jet spreads out
当反流束扩散时,测量位置在瓣膜下方距离太远,容易高估严重程度 - Central jets may overestimate (and conversely eccentric jets may underestimate) severity.
中央性反流束可能会高估(反之,偏心性反流束可能低估)严重性。
- Unpredictably expansion below the valve orifice potential source of error
# PISA or flow convergence
- This method is theoretically measurable (as in MR assessment)
该方法在理论上是可测量的 (如在 MR 评估中) - Has been shown to provide accurate quantification in severity of AR
已被证明可准确量化 AR 的严重程度 - However, NOT routinely practiced
然而,临床实践中用的并不多 - Limitations include suboptimal images in the presence of aortic valvular calcification and underestimation in aortic aneurysms. Validity is questionable for multiple/eccentric jets.
局限性包括在存在主动脉瓣钙化时的成像不佳,以及在主动脉瘤中被低估。对于多个 / 偏心性反流来说,有效性是值得怀疑的。
# Regurgitant Volume/Regurgitant Fraction/Regurgitant Orifice Area
Calculation:
- The volume of blood entering the LV via the mitral valve during diastole should equal the volume leaving the LV via the LVOT during systole (stroke volume).
舒张期经二尖瓣进入左室的血容量应等于收缩期经左室流出道的血容量(每搏量)。 - In AR, LV outflow exceeds mitral inflow since LVOT outflow also comprises blood that has entered the LV via AR during diastole.
在 AR 中,LV 流出量超过二尖瓣流入量,因为 LVOT 流出量还包括舒张期间通过 AR 进入 LV 的血液。 - in the absence of significant MR or a VSD
- The volume of blood entering the LV via the mitral valve during diastole should equal the volume leaving the LV via the LVOT during systole (stroke volume).
Volumetric Practical Method 容积实用方法
- Measure LVOT diameter in Parasternal long axis view
LVOT 径线测量和 AS 一样,胸骨旁长轴主动脉瓣局部放大 - Measure VTI using PW Doppler in Apical 5- chamber view
速度时间积分在心尖五腔使用 PW 进行测量
- Measure MV annulus diameter in Apical 4-chamber view
心尖四腔测量二尖瓣瓣环内径(舒张期 MV 打开时测量) - Measure VTI using PW Doppler in Apical 4-chamber view at mitral annulus level
PW 放置在二尖瓣瓣环水平,同内径测量水平,不是瓣尖
- Measure LVOT diameter in Parasternal long axis view
Other calculations
Regurgitant Fraction 反流分数
Regurgitant Orifice Area is the average size of the orifice in the aortic valve during diastole through which regurgitation occurs.
反流口面积是舒张期发生反流的主动脉瓣口的平均大小。
| Severity of AR (BSE Education Comittee Guidelines for Valve Quantification) | |||
|---|---|---|---|
| Mild | Moderate | Severe | |
| VC width (cm) | < 0.3 | > 0.6 | |
| Jet width/LVOT diameter (%) | < 25 | > 65 | |
| Regurgitant Volume (ml/beat) | < 30 | 31 - 59 | ≥ 60 |
| Regurgitant Fraction (%) | < 30 | 31 - 49 | ≥ 50 |
| Regurgitant Orifice Area (cm2) | < 0.10 | 0.11 - 0.29 | ≥ 50 |
VTI diastolic flow reversal (cm) | 15 | ||
| Pressure Half Time (ms) | > 500 | < 250 | |
尽量都测量,以综合评估
# Aortic Regurgitation Management
Mild - Follow up (2y echo)
Moderate
- Asymptomatic: Medical + 1-2 y echo
- Symptoms: Surgical
No evidence for vasodilators
没有用血管舒张药的证据Severe
- Surgical + assess cause: 病因评估
- Valve
- Valve + root
- Ascending aorta + resuspension
- Surgical + assess cause: 病因评估
# Surgical Indications
- Acute symptomatic AR 急性症状性反流
- Chronic severe AR: 慢性重度反流
- Symptoms 有症状
- Asymptomatic patients with LVEF ≤ 50%
LVEF ≤ 50% 的无症状患者 - Asymptomatic patients with LVEF > 50% and severe LV dilation (LVEDD > 70mm, LVESD > 50mm)
无症状,LVEF > 50% 且左心室严重扩张 (LVEDD>70 mm,LVESD>50 mm) - Patients undergoing other surgery (CABG, ascending aorta, other valvular).
接受其他手术 (CABG、升主动脉、其他瓣膜) 的患者。
- Regardless of severity of AR, patients with aortic root disease:
无论 AR 的严重程度如何,主动脉根部疾病:- Aortic Root > 45mm in Marfan's syndrome
马凡综合征患者的主动脉根部 > 45 mm - Aortic Root > 50mm in Bicuspid valves
二叶式主动脉根部 > 50mm - Aortic root > 55mm in other patients.
其余患者主动脉根部 > 55 mm
- Aortic Root > 45mm in Marfan's syndrome