# Echocardiography measure LV function
# Advantages
- Direct imaging = possible to make visual rather than mathematical assessment
直接成像 = 可以进行视觉评估而不是数学评估 - Relatively inexpensive equipment
相对便宜 - Fairly quick to perform and to analyse
相当快地执行和分析 - Not distressing to the patient
不会让病人感到痛苦 - No need to use radiation.
没有辐射
# Disadvantages
- Operator dependent
依赖于操作人员 - Poor image quality makes measurements difficult
图像质量差导致测量困难 - COPD, obesity
慢阻肺和肥胖 - LV wall motion abnormalities affect accuracy
左室壁运动异常影响准确性 - Prior myocardial infarction, cardiomyopathy.
既往心肌梗死、心肌病
# Requirements
- Good Long Axis, 4 Chamber and 2 Chamber views
良好的长轴、四腔观和两腔观 - Patience 耐心,需要多次尝试,配合患者呼吸等
- If you cannot take the images, the technology will fail.
如果无法采集到图像,则检查将失败。
# The four basic views
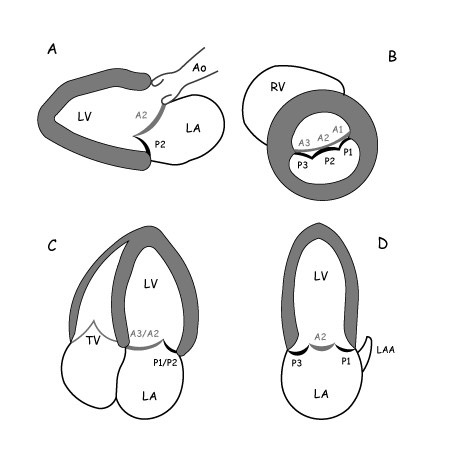
- LAX
- 室间隔和左室的下侧壁要处于水平状态
- SAX
- 心室要呈正圆形
- 4C 和 2C
- 要显示到心尖的部分
- 室间隔、房间隔与瓣环水平呈十字交叉
- 2C
- 要避免右室出现,否则角度不对




# Methods for global LV dysfunction 评价整体的左室功能障碍
- Linear measurements 线性测量
- e.g M-mode echocardiography
- 2-D measurements
- Fractional shortening
- Simpson's rule
- Doppler measurements
- Tei Index
- Emerging (for a long time!) measurements
# Linear measurements 线性测量
- M-mode echocardiography
有较高的可重复性 - Significant limitation: The beam frequently traverses the LV in a tangential manner. It often overestimates the true dimension.
显著的局限性:超声束经常以切线方式穿过 LV。对切线的角度有依赖,比如取样线要尽量与室间隔呈垂直状态,否则会导致径线测量被高估。
# 2D measurements 二维测量
- Improved compared to M-mode
与 M 模式相比有所改进 - Weakness: LV wall motion abnormalities
弱点:左室壁运动异常 - There are several, but few commonly used.
有几种,但常用的很少。
Fractional shortening
- Needs careful imaging
采集的时候需要仔细 - Performed well long axis view
尽量采集一个好的长轴切面 - Walls of LV need to be horizontal to the screen, and parallel to each other.
左室壁必须在屏幕上呈现水平,且室间隔和下侧壁要彼此平行。
- Needs careful imaging
Ejection Fraction
- It measures the volume of the LV
测量左室容积 - The 4 chamber apical view can suffice
心尖四腔切面就足够了 - The 2 chamber apical view can be added for increased accuracy (Biplane Simpson's)
可增加心尖两腔切面以提高精确度 (双平面辛普森) - End result: Ejection fraction
最终结果:射血分数 - Weakness: It relies on symmetric LV contraction
缺点:依赖于对称性的左室收缩 - It may need the use of LV contrast if poor endocardial definition.
如果心内膜清晰度差,可能需要使用左心室造影剂。
- It measures the volume of the LV
# Doppler-based techniques
- Tei-index 心肌做功指数
- Also called Myocardial Performance Index (MPI) 心肌综合指数
- 同时反应收缩功能和舒张功能的指标
- Main weakness of the technique: Arrhythmias with variable cardiac cycle length.
该技术的主要缺点:心律失常伴不同的心动周期长度时不适用。 - 不是临床常规方法,可以作为科研方法
# Tei-index calculation
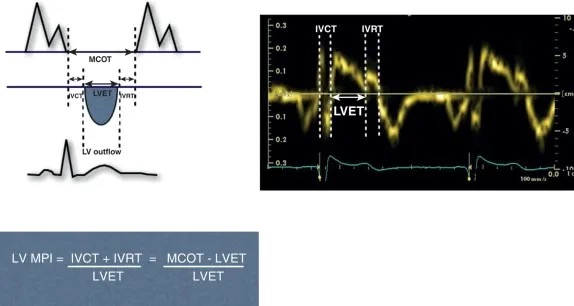
Myocardial performance (Tei) index obtained as the sum of isovolumetric contraction time ( IVCT ) and isovolumetric relaxation time ( IVRT ), divided by the LV ejection time ( LVET ).
心肌功能(Tei)指数为等容收缩时间(IVCT)和等容松弛时间(IVRT)之和除以左室射血时间(LVET)。MCOT, Mitral valve closure to opening time (msec).
MCOT,二尖瓣关闭至打开的时间(毫秒)。和右心的一样,可以用脉冲多普勒也可以用组织多普勒测量计算
| 参考值 | |
|---|---|
| Mean normal value | 0.39 ± 0.05 |
Dilated cardiomyopathy | 0.59 ± 0.10 |
Coronary artery disease with complications: chronic cardiac failure(CCF), arrhythmia, angina | 0.65 ± 0.2 |
应用不同的测量方法(PWD/TDI),Tei 指数的参考值也不同
# Emerging measurements
To be discussed in separate lecture (LV volume and mass)
# Methods for regional 评价节段性
# 16 or 17 segment model 节段模型
A lot of the newer software has switched to 17 segments.
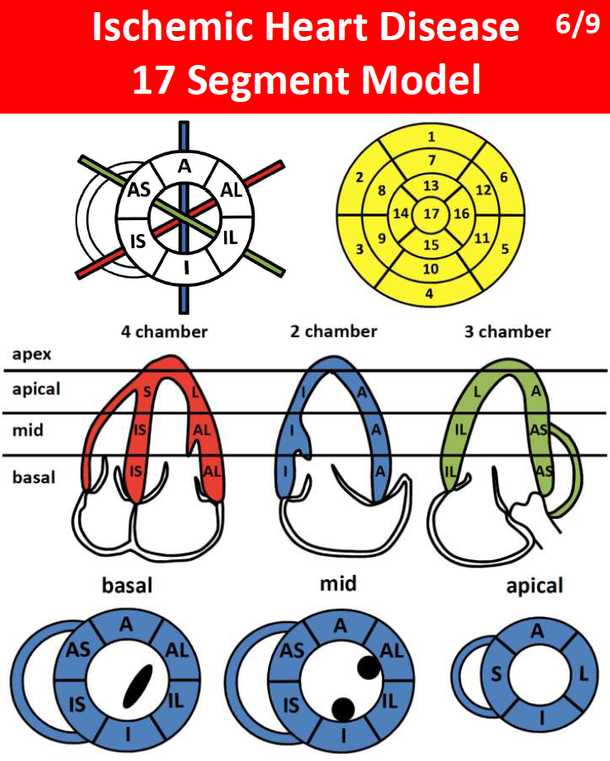
| Segments named | 节段命名 |
|---|---|
| Basal | 基底部 |
| Mid | 中部 |
| Apical | 心尖部 |
| Apex | 心尖帽 |
| A | 前壁 |
| AS | 前间隔 |
| IS | 后间隔 |
| I | 下壁 |
| IL | 后壁 |
| AL | 前侧壁 |
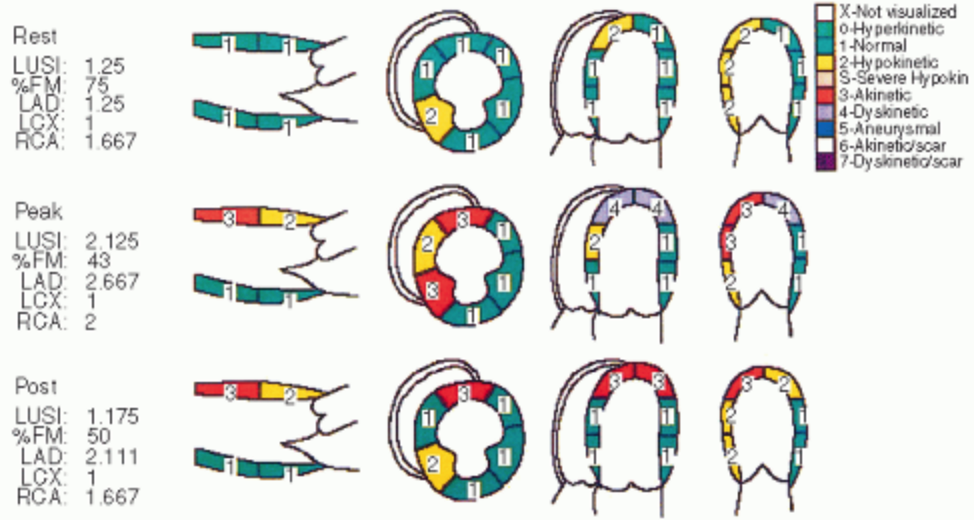
- An example of a stress echocardiographic report is provided, including a regional wall motion scoring summary.
负荷超声心动图报告的例子,包括节段性室壁运动评分总结。- LVSI, left ventricle score index; 左心室评分指数
- % FM, percentage of normally functioning segments; 正常功能段的百分比
- LAD, left anterior descending; 左前降支
- LCX, left circumflex; 左旋支
- MI, myocardial infarction; 心肌梗死
- RCA, right coronary artery. 右冠状动脉
| 运动计分 | ||
|---|---|---|
| X | not visualised | 不可视 |
| 0 | hyperkinetic | 运动功能亢奋 |
| 1 | normal | 正常 |
| 2 | hypokinetic | 运动功能减退 |
| 2 | severe hypokinetic | 重度运动功能减退 |
| 3 | akinetic | 运动不能 |
| 4 | dyskinetic | 反向运动 |
| 5 | aneurysmal | 室壁瘤 |
| 6 | akinetic with scar | 运动不能伴疤痕 |
| 7 | dyskinetic with scar | 反向运动伴疤痕 |
# Q&A
对舒张末 LVID 测量,长轴切面是测量二尖瓣瓣口处,还是左室最大内径处?比如有些老年人室间隔基底段肥厚,或是扩心病患者左室呈球形,可能左室最大舒张未内径就在左室中部,或是肥厚的室间隔基底段后方,有时偏差可能在 1cm,这种情况下怎么测量 LVID?
不管是存在肥厚型心肌病还是扩张型心肌病,测量的部位都是在二尖瓣瓣叶尖的位置,因为参考值都是以此为标准的。如果变异性非常大,那么可以不仅仅运用二维测量,还可以加上三维的测量,如 Simpson 双平面法测算容积。
CMR 是否也遵循一样的测量标准?
不是的,CMR 是基于对容积的分析,和心超不一样,CMR 对几何形态的依赖很小,不同的操作者或机器之间的测量差距较小。
心律失常(比如房颤)会影响 Simpson 方法的结果吗?
心律失常,如房颤,会影响 Simpson 方法。实践中很难从长短不齐的心动周期中选取一个代表心动周期。在存在房颤的时候,我们更偏向凭经验用目测来进行评估,结合多个测量指标用于参考,测量值并不是绝对的。