- Easy to get a quick measurement
- Very easy to make a sizeable mistake
- The trick is to know when a technique cannot be used.
诀窍是知道什么时候不能使用某项技术。
# Anatomy


- Inlet, apical trabecular and outlet portion
入口、心尖肌小梁 / 肉柱和出口部分 - These portions do not have discrete borders
这三个部分没有明确的界限;因此超声测量中用到的 Simpson 方法会用到一个几何学上的假设 - Thickest at base; only 1 to 2 mm at apex
心底部最厚;心尖部只有 1 到 2 毫米 - Myocardial strands oblique in the subepicardium, circumferential in the middle and longitudinal in the subendocardium.
心肌束在心外膜下倾斜,在心内膜下呈环状,在心内膜下呈纵向。因此也决定了心肌的收缩方向,有一定的旋转扭曲。 - LV movements:
- Radial (circumferential) thickening 环向 / 内向增厚
- Longitudinal shortening 纵向缩短
- Rotation 旋转
If the LV does not work well, it is not a single view or measurement type that gives us the answer.
如果左室功能不好,则不能使用单一的切面或评估方式,应综合多个方法进行全面的评估
# Normal LV measurements
| Women | Men | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Reference range | Mildly abnormal | Moderately abnormal | Severely abnormal | Reference range | Mildly abnormal | Moderately abnormal | Severely abnormal | |||
| Linear method 线性方法 | ||||||||||
Endocardial fractional shortening, % | 27-45 | 22-26 | 17-21 | ≤16 | 25-43 | 20-24 | 15-19 | ≤14 | ||
Midwall fractional shortening, % | 15-23 | 13-14 | 11-12 | ≤10 | 14-22 | 12-13 | 10-11 | ≤10 | ||
| LV mass 左室质量 | ||||||||||
| LV mass, g | 67-162 | 163-186 | 187-210 | ≥211 | 88-224 | 225-258 | 259-292 | ≥293 | ||
| LV mass/BSA, g/m2 | 43-95 | 96-108 | 109- -121 | ≥122 | 49-115 | 116-131 | 132-148 | ≥149 | ||
| LV mass/height, g/m | 41-99 | 100-115 | 116-128 | ≥129 | 52-126 | 127-144 | 145-162 | ≥163 | ||
| LV mass/height2, g/m2 | 18-44 | 45-51 | 52- -58 | ≥59 | 20-48 | 49-55 | 56-63 | ≥64 | ||
| Relative wall thickness, cm | 0.22-0.42 | 0.43-0.47 | 0.48-0.52 | ≥0.53 | 0.24-0.42 | 0.43- -0.46 | 0.47-0.51 | ≥0.52 | ||
| Septal thickness, cm | 0.6-0.9 | 1.0-1.2 | 1.3-1.5 | ≥1.6 | 0.6-1.0 | 1.1-1.3 | 1.4-1.6 | ≥1.7 | ||
| Posterior wall thickness, cm | 0.6-0.9 | 1.0-1.2 | 1.3-1.5 | ≥1.6 | 0.6-1.0 | 1.1-1.3 | 1.4-1.6 | ≥1.7 | ||
| 2D Method 二维方法 | ||||||||||
Ejection fraction, % | ≥55 | 45-54 | 30-44 | <30 | ≥55 | 45-54 | 30-44 | <30 | ||
| LV dimension 左室尺寸 | ||||||||||
LV diastolic diameter | 3.9- 5.3 | 5.4-5.7 | 5.8-6.1 | ≥6.2 | 4.2-5.9 | 6.0-6.3 | 6.4-6.8 | 26.9 | ||
LV diastolic diameter/BSA, cm/m2 | 2.4-3.2 | 3.3-3.4 | 3.5-3.7 | ≥3.8 | 2.2-3.1 | 3.2-3.4 | 3.5-3.6 | ≥3.7 | ||
LV diastolic diameter/height, cm/m | 2.5-3.2 | 3.3-3.4 | 3.5-3.6 | ≥3.7 | 2.4-3.3 | 3.4-3.5 | 3.6-3.7 | ≥3.8 | ||
| LV mass 左室质量 | ||||||||||
| LV mass, g | 66-150 | 151-171 | 172-182 | >193 | 96-200 | 201-227 | 228-254 | >255 | ||
| LV mass/BSA, g/m2 | 44-88 | 89-100 | 101-112 | ≥113 | 50-102 | 103-116 | 117-130 | ≥131 | ||
BSA, body surface area 体表面积;LV, left ventricular; 2D, 2 dimensional.
记住绿色的,尤其是正常值的范围
- 缩短分数仅仅是单平面的二维测量,当存在左室收缩功能障碍时,并不能很好的反映实际情况。比如在胸骨旁长轴的径线测量,如果收缩功能异常正好出现在下壁,心尖两腔下测得的 FS 很可能偏高。
- Simpson 双平面法测得的 EF 是目前的金标准。参考值不同协会或地区略有不同。
- 左室舒张内径除以体表面积后,男女差异显著减小;需要考虑到身高体重的影响
# Linear method 线性测量方法
有两种:
- M-mode M 模式
- 2D Fractional Shortening 二维缩短分数
局限性:
- If there are LV wall motion abnormalities, they are always inaccurate.
如果有左室壁运动异常,它们总是不准确的。 - Rely on symmetrical contraction of the myocardium.
依赖于心肌的对称性收缩。 - Operator-dependent.
操作者主观影响大
# M-Mode
# MAPSE
- Annular motion towards apex 瓣环向心尖部的移位
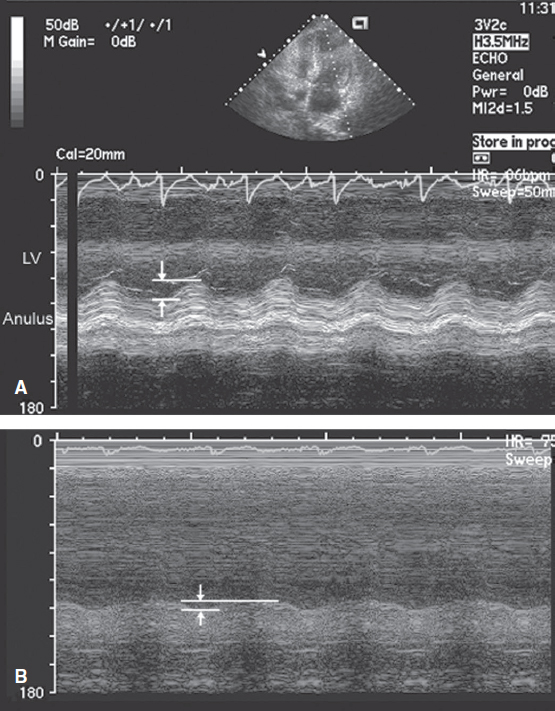
- Apical view recorded in two patients demonstrates the measurement of the descent of the base with M-mode echocardiography (arrows).
两名患者的心尖四腔心显示了 M 型超声心动图测量基线值的下降。 - The M-mode interrogation beam has been directed from the apex of the heart through the lateral annulus.
选择 M 模式,把取样线放置在二尖瓣瓣环,超声波束从心尖到左室侧壁的瓣环处。 - A: Note the approximate 1.6 cm of annular motion toward the apex in systole.
收缩期,二尖瓣瓣环向心尖方向移动约 1.6cm。(评估左室纵向的收缩功能) - B: Recording in a patient with severe systolic dysfunction reveals substantially decreased annular motion of <1.0 cm in systole.
严重的收缩期功能障碍患者,收缩期瓣环运动显著减弱,幅度非常小,朝心尖移动距离<1.0 cm。
该方法可以称为 MAPSE, Mitral annular plane systolic excursion,评估左室的纵向收缩功能,如果运动降低,提示左室僵硬度高,比如心肌淀粉样变、左室肥厚,都有可能出现纵向收缩功能障碍。
# EPSS
- E-point septal separation E 峰间隔距离
- Maximal early opening of mitral valve (E-point) distance from IVS 二尖瓣的最大早期打开点(E 峰)与 IVS 距离
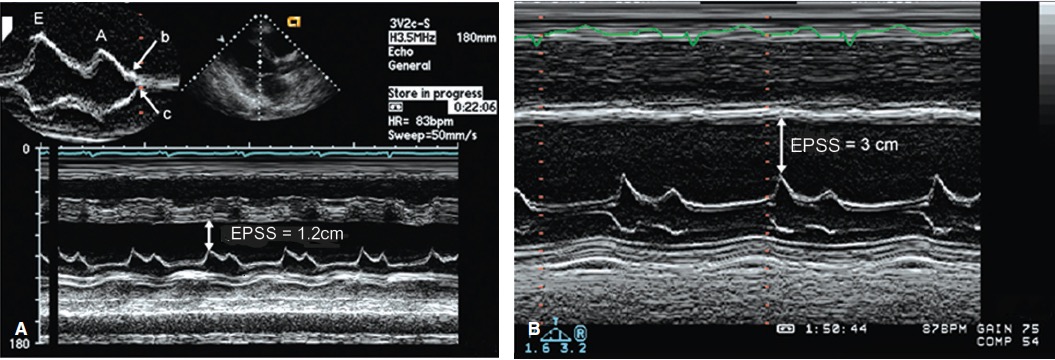
M-mode echocardiograms recorded in two patients with significant systolic dysfunction.
在两名具有明显收缩功能障碍的患者中记录了 M 型超声心动图。胸骨旁左室长轴切面,M 模式采样线放在二尖瓣的前叶上;描绘出二尖瓣前叶随着时间变化的运动曲线;
The magnitude of opening of the mitral valve, as reflected by E-wave height, correlates with the volume of transmitral flow and, in the absence of significant mitral regurgitation, with left ventricular stroke volume.
在收缩期,二尖瓣运动的 E 峰应靠近室间隔,E 波峰值顶点反映了二尖瓣的打开度,与二尖瓣血流量相关,在没有明显二尖瓣返流的情况下,与左心室每搏量相关。The internal dimension of the left ventricle correlates with diastolic volume. As such, the ratio of mitral excursion to left ventricular size parallels ejection fraction.
左心室的内部尺寸与舒张体积相关。因此,二尖瓣偏移与左心室大小的比率与射血分数平行。Normally, the mitral valve E-point (maximal early opening) is within 6 mm of the left side of the ventricular septum. In the presence of a decreased ejection fraction, this distance is increased.
通常,二尖瓣 E 峰(最大早期开口)距离心室隔左侧 6mm 以内。在射血分数降低的情况下,这个距离会增加。A: An E-point septal separation (EPSS) of 1.2cm (normal, <6mm).
图 A:E 峰间隔距离(EPSS)为 1.2cm(正常,<6mm)。B: Recording in a patient with more significant left ventricular systolic dysfunction in which the EPSS is 3.0cm.
图 B:左室收缩功能障碍更严重的患者,EPSS 为 3.0cm,提示二尖瓣前叶根本没有接近室间隔Also note the interrupted closure of the mitral valve with a B bump (top), indicating an increase in the left ventricular end-diastolic pressure.
另需注意二尖瓣关闭中断,并伴有 B 峰 (顶部),表明左室舒张末压升高。此方法目前已经比较少用
# 2D Fractional Shortening
局限性:
- 如果存在左室收缩节段性异常,可能导致测量误差。如心尖四腔心可以观察到节段性收缩功能障碍,但在胸骨旁长轴切面测量的值为正常,无法体现节段性异常。
- 心肌有三个不同的收缩方向,FS 仅体现了一个内向的环向运动,不能很好体现其纵向以及扭转的功能。
- 胸骨旁长轴可以看到前间隔,但如果心尖两腔下前壁出现的功能障碍,FS 无法很好的体现左室功能
- 而 EF 是 FS 的两倍,如果 FS 存在误差,则 EF 是两倍的误差
因此,临床上很少用 FS 乘 2 来计算 EF
- Fractional Shortening Measurement :
| 参考范围 | |
|---|---|
| < 29% | LV systolic dysfunction |
- Ejection Fraction Measurement:
| 参考范围 | |
|---|---|
| 55-65% | normal |
| 45-55% | mildly impaired |
| 35-45% | moderately impaired |
| <35% | severely impaired |
# Pitfalls 隐患
可能导致测量误差的陷阱:
- Off-axis images 图像离轴
图片偏离中心轴时,如果进行 M 模式测量,取样线不能很好的和室间隔垂直,可能导致误差 - “In-between views”
在应用心尖四腔测量时,有可能切到四腔心和五腔心或者和三腔心之间,这些情况下可能出现较大测量误差。 - Foreshortened chambers 腔室缩短
在应用心尖四腔测量时,有时不能很好的切到心尖部位,可能导致出现心尖透视缩短。在进行心尖视窗检查时,要选择心尖搏动最明显处,尽可能下降一个肋间,尽量避免心尖透视缩短的问题 - Poor definition 清晰度不高
在做径线测量时,成像质量越好,心内膜界限越清晰,测量结果越精确。有些慢阻肺或者肥胖的患者,图像清晰度会差,心内膜显影不清,很难找到正确的边界。如果找不到明确的边界,就不应该追踪测量,因为不会得到准确的测量值。 - Wall motion abnormalities 室壁运动异常
胸骨旁长轴切面进行单一平面评价时,只会考虑间隔和后壁的收缩情况,而忽略其他的一切;因此尽量不采用,而是多使用 Simpson 双平面法或者三维的方法进行综合评估。 - If it does not look right = do not measure it!
# 2D method 二维方法
# Effort for improvement
- 2 dimensional image measurements
- More information = more assurance 信息越多越精确
- Many exist, we essentially use only one.
有很多种,目前基本上只用了一种。
当二维测量存在困难或误差时,也可以考虑其他方法
一般运用多种方法,方法越多,侧量越全面
# 2D method weakness
- Same as in linear 二维方法和线性测量存在相似的缺点
- Rely on symmetrical LV contraction
依赖对称性的左心室收缩 - Require good endocardial definition
需要良好的心内膜边界清晰度- Solution: LV contrast
解决办法:左室增强剂
- Solution: LV contrast
- Operator dependent.
对操作者水平的依赖
- Rely on symmetrical LV contraction
# LV systolic function

- Top: The methodology for determining fractional area change, which is defined by the formula in the figure.
顶图:图中的公式定义了面积变化分数的确定方法 - Middle and bottom: Using the geometric assumption that the left ventricular cavity represents a cylinder and cone configuration, the volume of each separate component can be calculated as noted. The overall left ventricular volume equals the sum of the two volumes.
中图和底图:使用几何假设,即左室腔代表下方的圆柱体和上方的圆锥体结构,可以如上所述单独计算两个部分的体积。左心室总容积等于两个部分的容积之和。
# Simpson 方法
就是把这上述的两个部分,再细分为数个等高的圆盘。重要的参数包括:圆盘的半径和高度。整体的高度是左室心尖到二尖瓣瓣环。
The operator just needs to delineate the endocardium in the 4C and 2C views in systole and diastole.
操作者只需要在 4C 和 2C 切面上,在收缩末期和舒张末期进行心内膜描绘。The machine does the mathematics:
机器讲进行数学运算:- The LV cavity is arbitrarily decided into 10 segments of equal height.
左室腔被任意确定为 10 个高度相等的部分。 - The height of each cylinder is defined as the overall length divided by the number of disks.
每个圆柱体的高度定义为总长度除以圆盘数。 - The total volume of the ventricle is the same of the individual disk volumes.
心室总容积与圆盘容积之和相同。
- The LV cavity is arbitrarily decided into 10 segments of equal height.
与面积变化分数运用面积有点类似,此处运用了容积
- 心尖两腔心展示了(右侧)前壁和(左侧)下壁
- 心尖四腔心展示了(前外侧)游离壁和(后侧)室间隔
同样依赖清晰度,看不清楚心内膜边界时不用,否则误差大
# LV Volume & Mass
Initial calculations by M-mode
最初是用 M 模式进行计算Usual M-mode problems
M 模式存在局限性They assume predetermined geometry
假设了左室为一个预定的几何形状If the LV shape is abnormal, they lose accuracy.
如果左室形状异常,则将影响测量的精确度。Improvement of 2D echocardiography 使用下面的方法,二维测量将较单纯的 M 模式得到改善
- One method is the Teichholz (cubed) formula (which can be used in M-mode as well)
一种方法是 Teichholz(立方体)公式(也可以在 M 模式中使用) - It assumes that the LV is a sphere
假设左室是一个球体 - The diameter is the internal diameter of the LV and the sphere thickness is the myocardial thickness.
球体的直径为左室内径,球体的厚度为心肌厚度。
- One method is the Teichholz (cubed) formula (which can be used in M-mode as well)
LV mass from cubed formula
# Q&A
LV 测量表格中,Linear method 中 FS 分为 Endocardial FS 和 Midwall FS,有什么不同呢?
测量 FS 时,我们通常是在胸骨旁左室长轴测中间位置的心肌边缘的距离,也就是心内膜 Endocardial FS;Midwall FS 是指测量心肌中间部位的距离,这不是目前常规的做法,是学术或过时的做法,现在也不会单独使用。
Volume of LV = Myocardial volume?
No, 计算 LV mass 的公式中的 Volume of LV / LV volume 其实是心外膜为边界的所有的体积之和,包含了心肌、血池容积
Myocardial volume 只是心肌的体积