# 2D and M mode Echocardiography
# 2D echocardiography
最常用的成像模式
- Real time views of the heart in motion
心脏运动的实时视图- Morphology and functional assessment
形态学和功能评估 - Guides other modes e.g. M mode
引导其他模式,例如 M 模式
- Morphology and functional assessment
- Electrocardiogram(ECG) gated clips stored
存储心电门控剪辑 - Frozen images for measurement on or offline.
冻结图像以进行在线或离线测量。
# M mode M 模式
- Display of motion related changes in time along a single line
沿单一扫查线,随时间变化成像组织的运动变化 - High TEMPORAL resolution
高时间分辨率 - Use 用于
- MOTION TRACKING AND TIMING
运动跟踪和计时;对运动物体的追踪、描述 - MEASUREMENTS - if line is PERPENDICULAR to measured structure.
测量 - 如果扫查线垂直于测量结构。
比如室间隔、心室的径线测量,要求是取样线与所测结构呈垂直状态,这样不会高估。比如室间隔的厚度,分别采取垂直取样和倾斜取样,倾斜取样有可能会高估室间隔的厚度,有可能误诊断为左室肥厚。
- MOTION TRACKING AND TIMING
# Windows 声窗
- Parasternal windows 胸骨旁声窗
- Left decubitus position; 左侧卧位;左臂高举
- 3-4th intercostal space 胸骨旁左侧第 3~4 肋间隙

- Apical windows 心尖声窗
- Left decubitus position; 左侧卧位;
- Apex pointing to right. 顶点指向右侧。

- Subcostal windows 剑突下声窗
- Supine position; 仰卧位
- knees flexed; 屈膝
- Transducer in mid-epigastric position. 探头放置腹上部中间位置
- Supine position; 仰卧位
- Suprasternal windows 胸骨上窝声窗
- Supine with chin up; 仰卧,下巴上抬
- transducer in suprasternal notch. 胸骨上切迹放置传感器。
- Supine with chin up; 仰卧,下巴上抬

绝大多数患者通过以上四个声窗都可以得到完整的经胸超声心动图的成像,但是如果患者存在主动脉瓣狭窄,一般也会运用到右侧胸骨旁声窗。
- Right parasternal windows 右胸骨旁声窗
- Lying on right side decubitus 右侧卧位,右臂上抬
- Mainly for aortic stenosis for velocity rather than imaging. 主要针对主动脉瓣狭窄的血流速度而不是成像。

# Views
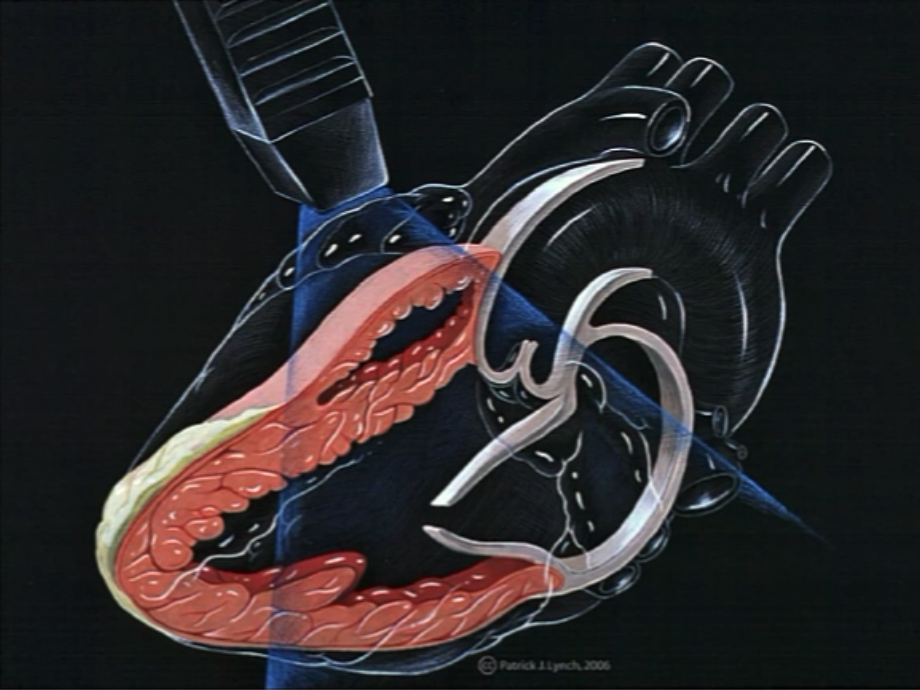
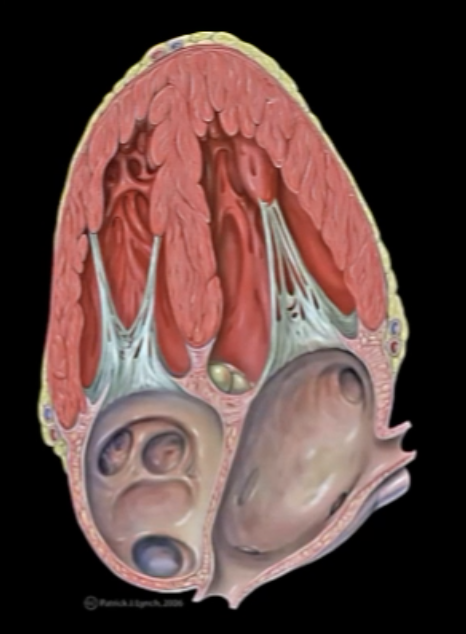
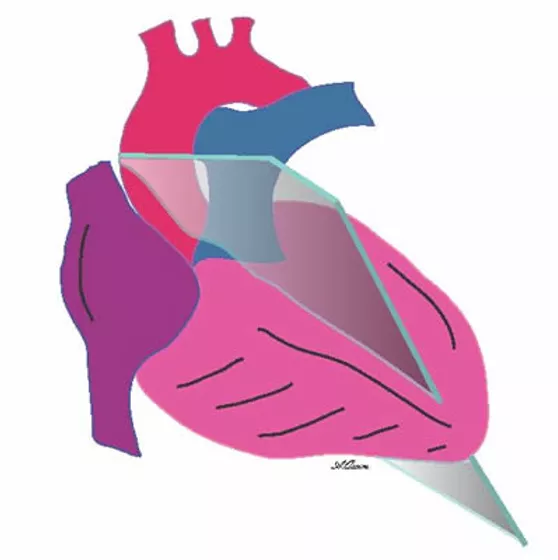
# Parasternal Long axis (PTLAX) 胸骨旁长轴
 胸骨旁长轴")
| PTLAX: parasternal long axis | 胸骨旁长轴 |
| Aorta | 主动脉 |
| Aortic valve | 主动脉瓣 |
| Conus arteriosus | 动脉圆锥 / 筛漏斗 |
| RV: right ventricle | 右心室 |
| Interventricular septum | 室间隔 |
| LV: left ventricle | 左心室 |
| Posterior (infero-lateral )wall, LV | 左室后壁 |
| MV: mitral valve | 二尖瓣 |
| LA: left atrium | 左心房 |
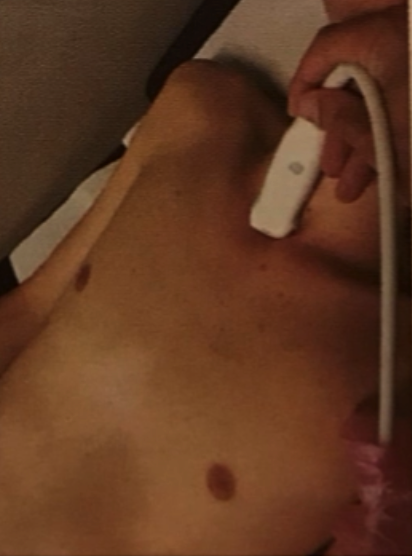
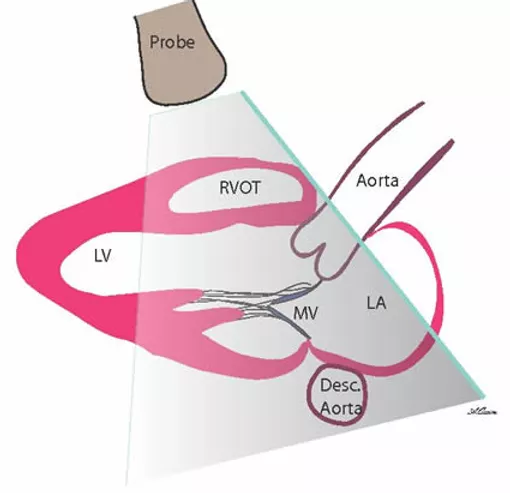
# Standard Parasternal Long Axis View 标准胸骨旁长轴切面

- Place the transducer just left of the sternum in the 4th or 5th intercostal space.
将探头放在胸骨左缘第 4 或第 5 肋间 - The transducer marker should be facing the right shoulder.
探头标记应该朝向右肩
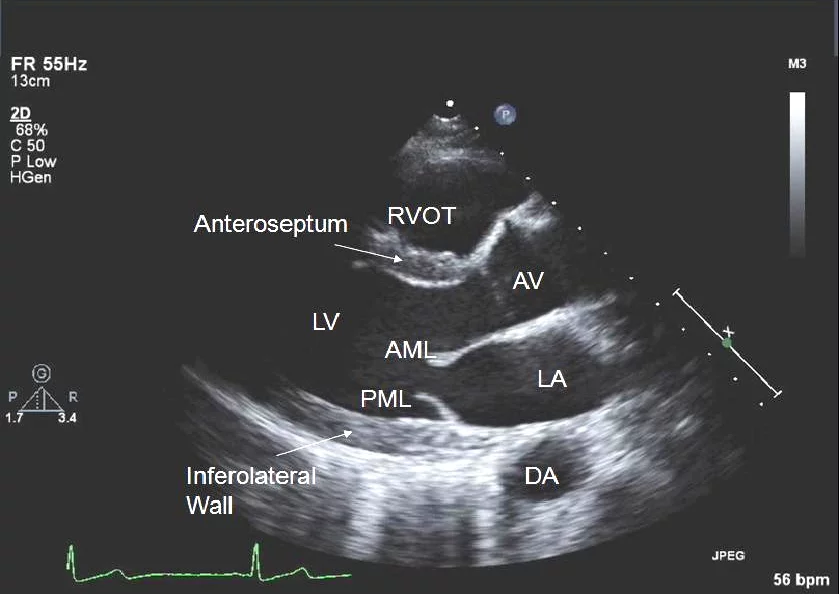
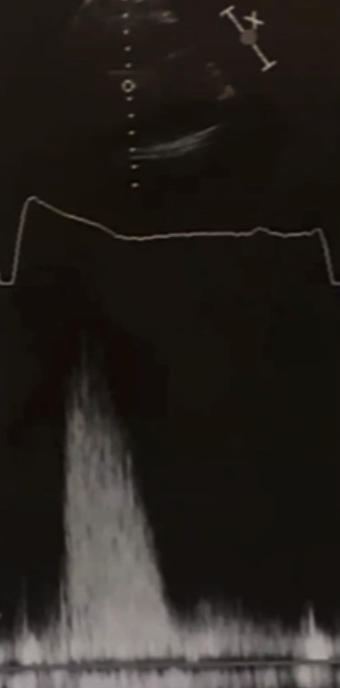
# Measurement from PTLAX 测量
- 二维成像中,看不到心尖,只能看到 2/3 左右的心腔;另一端可以看到部分主动脉根部
- 一般要求二维成像的室间隔还有主动脉部分,应该成一个水平状态,这样运用 M 模式进行测量的时候,才能保证到测量值相对比较精确。
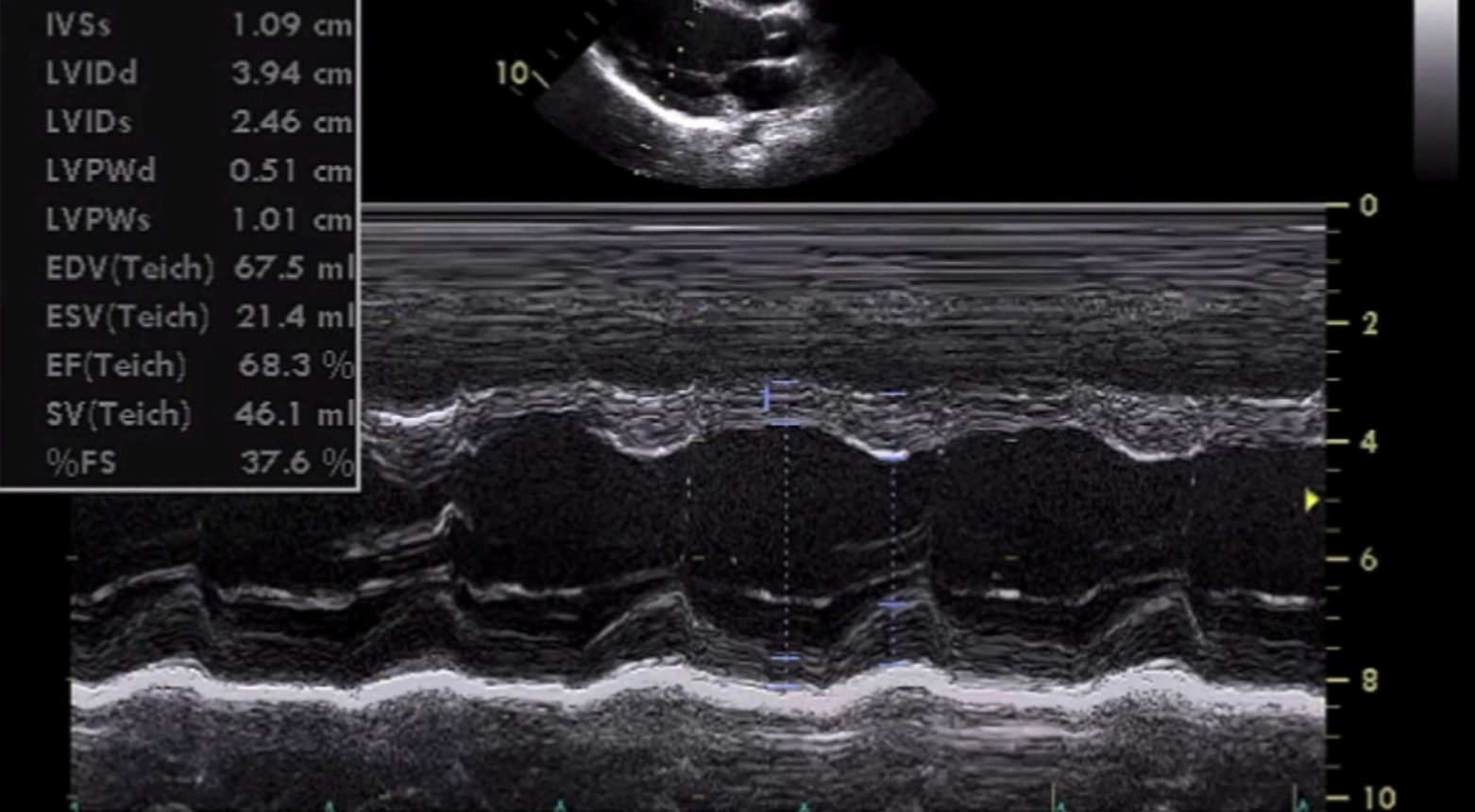
- 二维成像图中间的线性结构为【取样线】,一般放在二尖瓣瓣叶尖的位置。下方就会呈现取样线随着时间变化的图像,大概记录了 5-6 个心动周期,可以在此进行径线的测量。最下方有心电图,可以看到 QRS 波,可以给予时间上的指引。在舒张末期,可以进行室间隔厚度、左室内径、后壁的测量;在收缩末期,可以进行左室内径的测量。当进行了这些径线测量之后,系统就会自动算出左室舒张末收缩末的容积,以及射血分数、短轴缩短率。
- 目前在临床已经较少运用 M 模式了,会更多的运用二维测量。把动态图分别静止在舒张末期和收缩末期,来进行二维测量。系统也会根据所测得的结果,自动算出射血分数、短轴缩短率。
- 为什么现在 M 模式不太常用呢?是因为成像的时候,取样线的位置很难真正做到和室间隔呈垂直状态,就会使得测量值出现很大的误差。比如没有真正垂直时,会使室间隔的厚度偏大,有可能得到左室肥厚的错误诊断。
- 所以在实际操作中,要根据具体的成像来选择二维或者是 M 模式来进行测量。
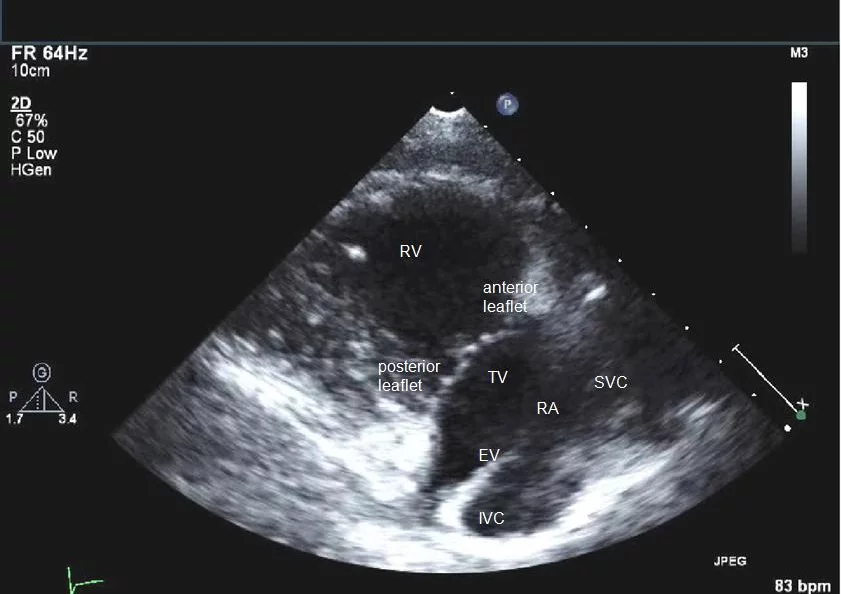
# PTLAX - RV views (RV Inflow view & RV Outflow view)
在胸骨旁长轴的基础上,保持探头与心脏相同的方向,可以进行倾斜:

- Tilt probe caudally
倾斜探头,使超声波束指向下方- RV inflow
RV 流入道 - Tricuspid valve
三尖瓣
- RV inflow


- Tilt probe cranially
倾斜探头,使超声波束指向上方- Pulmonar valve and RV outflow tract
肺动脉瓣和 RV 流出道
- Pulmonar valve and RV outflow tract
# Parasternal Short axis (PTSAX) 胸骨旁短轴
")
| Anterior wall | 前壁 |
| Lateral wall | 侧壁 |
| Inferior wall | 下壁 |
| Anterior papillary muscle | 前外乳头肌 |
| Posterior papillary muscle | 后内乳头肌 |


- Rotate the probe 90 degrees clockwise from the parasternal long axis.
在胸骨旁长轴的基础上,对探头进行顺时针 90° 的旋转,就可以得到胸骨旁短轴切面。 - The transducer marker should be facing the left shoulder now
探头标记应该朝向左肩 - There are multiple levels of short axis images depending on how you tilt the probe.
根据探头的倾斜方式,有多个级别的短轴图像。 - The slices show the LV from the base to apex and all four valves.
切片显示从左室底部到顶部以及所有四个瓣膜。
Now we are cutting heart like a cylinder and depending on the ANGULATION we can see the following structures
Starting from the most cranial and moving caudally the following views are seen.
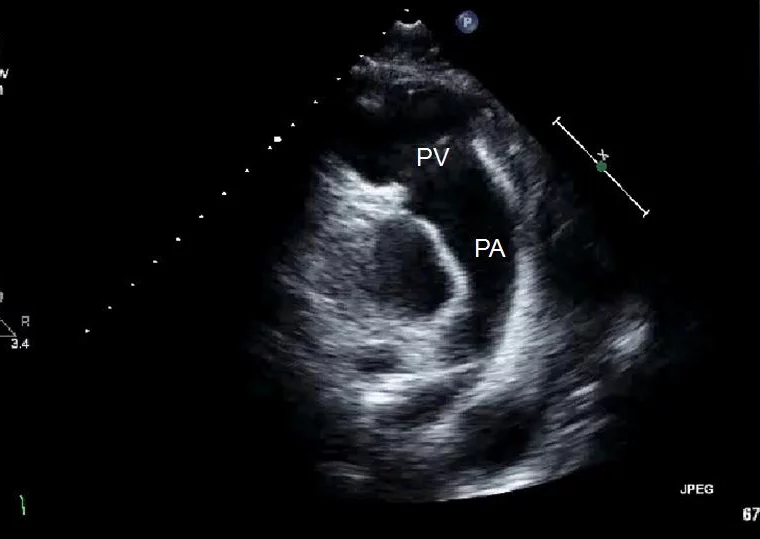
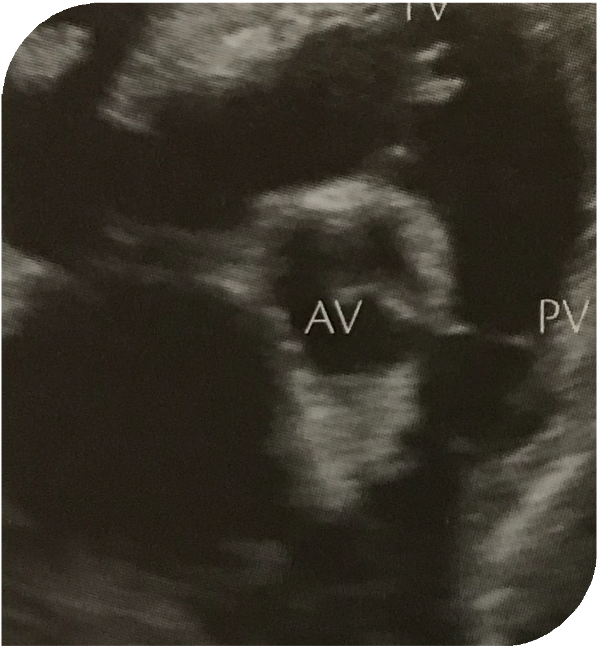
# RV outflow tract 右室流出道
- Note probe may need to be moved caudally fromthe classic on-axis position of PTLAX
注意:探头可能需要从 PTLAX 的经典轴上位置向尾部移动
- 这是胸骨旁短轴右室流出道的成像,最上方可以看到右室室壁,中间是右室流出道,右下方的瓣膜是肺动脉瓣,肺动脉瓣的下方是肺主动脉以及分支。
- 通过这个成像可以评估右室的收缩功能,也可以评估肺动脉瓣有没有存在狭窄或反流。
- 肺主动脉分支的部位,可以加上彩色多普勒,检查有没有动脉导管未闭的情况。

- Slight angulation superiorly will show the pulmonary artery and sometimes past the bifurcation.
稍向上成角可显示肺动脉,有时可越过分叉。 - This is the view that is useful for seeing a PDA with color Doppler (usually a jet seen along the left PA).
这是一个有助于用彩色多普勒观察 PDA 的切面(通常是沿着左 PA 看到的喷射)。 - Also note the geometry of the pulmonary valve and artery, more anterior and almost perpendicular to the aortic valve plane.
还要注意肺动脉瓣和肺动脉的几何形状,更靠前,几乎垂直于主动脉瓣平面。 - It is important to use PW Doppler above and below the pulmonic valve. Sometimes PW Doppler can be done separately in each pulmonary artery branch if stenosis or a mass is seen.
重要的是在肺动脉瓣上下使用 PW 多普勒。有时,如果发现狭窄或肿块,可以在每个肺动脉分支单独进行 PW 多普勒检查。 - Note that this individual is in atrial flutter during the echocardiogram.
注意,该患者在超声心动图检查期间出现心房扑动。 - PA - pulmonary artery, PV - pulmonic valve
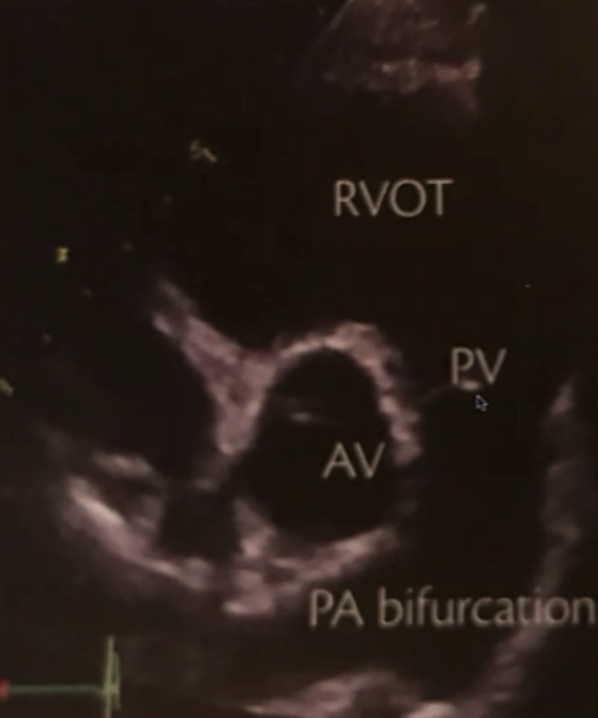
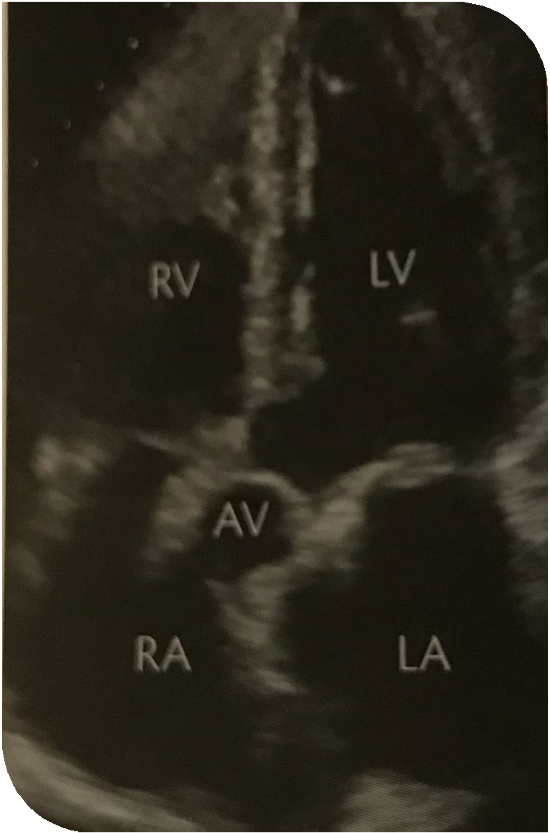
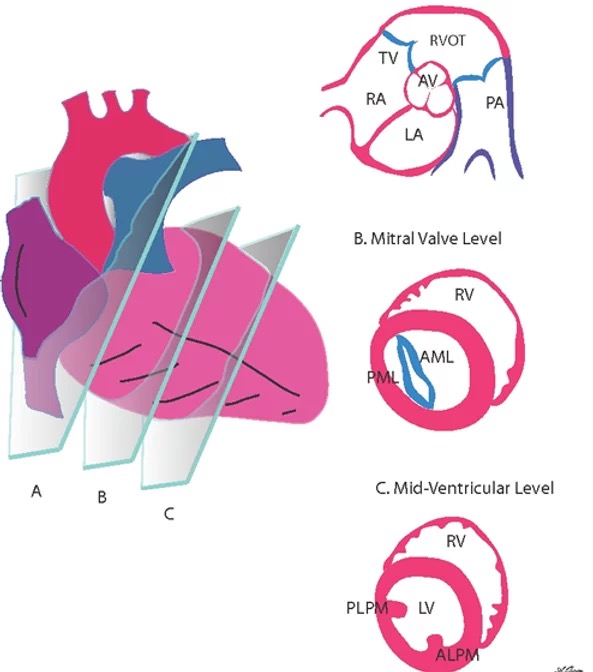
# Great Vessels Level
- The view can be used toobtain an M-Mode of the Aorta and left atrium for measurement of aortic sinuses and AP left atrial diameters.
该切面可用于获得主动脉和左心房的 M 型图像,用于测量主动脉窦和左房内径。
- 居中的就是主动脉瓣,有三个瓣叶,最上方的是右冠瓣,左侧的是无冠瓣,右侧的是左冠瓣。主动脉瓣的下方是左房,左房的左侧是房间隔。
- 该切面下可以评估主动脉瓣有没有存在狭窄,如果加了彩色多普勒,也可以评估有无主动脉瓣反流。
- 加上 M 模式,放置取样线通过右室流出道、主动脉瓣,则可以测量右室流出道的内径、主动脉根部的径线测量,以及在收缩末期测量左房的前后径。

- It is quite useful to zoom in on the aortic valve to try to assess whether it is trileaflet.
Zoom 放大主动脉瓣对评估其是否为三叶瓣非常有用。 - Color Doppler here can also help tell the origin of a regurgitant jet.
彩色多普勒也可以帮助判断返流的起源。 - The cusps can always be identified as follows, whether in this view, the subcostal view or via TEE:
无论是在该切面中,还是在剑突下切末中,还是在经食管超声心动图(TEE)上,都可以按照以下方式确定瓣叶:
the intra-atrial septum always intersects the non coronary cusp; the right coronary cusp is the most anterior and abuts the right ventricular outflow tract. The left coronary cusp is therefore the one that is left.
房间隔始终与无冠窦相交;右冠瓣位于最前方,毗邻右心室流出道。因此,剩下的那个瓣叶则是左冠瓣。
Sometimes slight angulation will allow visualization of the left main and right coronary arteries.
有时轻微的角度可以显示左主干和右冠状动脉。 - RCC - right coronary cusp, LCC - left coronary cusp, NCC - non coronary cusp.

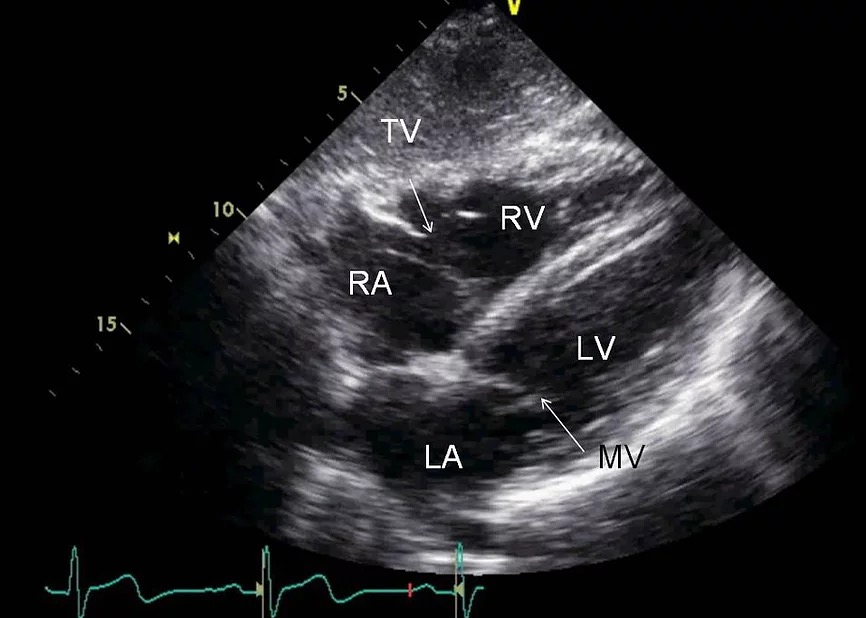
This is the most basal short axis view that lays out the 2 atria, 3 valves and the RV outflow tract.
这是最基本的短轴视图,显示了 2 个心房、3 个瓣膜和 RV 流出道。Repeat PW and CW across the tricuspid valve is usually done here.
三尖瓣 PW 和 CW 通常在这里完成。TV - tricuspid valve, RA - right atrium, LA - left atrium, AV - aortic valve, PV - pulmonary valve, RVOT - right ventricular outflow tract, PA - pulmonary artery.
图中是一个三叶式的主动脉瓣,可以在图像上来评估是否是二叶瓣、检查活动性、有无钙化、有无狭窄。加上彩色多普勒之后,也可以看有没有主动脉瓣反流。
主动脉瓣的左侧是三尖瓣,右侧是肺动脉瓣,下方是左房
左房容积在心动周期的不同时相上有很大的变化,一般在收缩末期进行左房内径的测量。
房间隔的部位,左侧是右房,右侧是左房。存在这个房间隔缺损的时候,加上彩色多普勒可以发现心内分流的情况。
# Mitral Valve Level
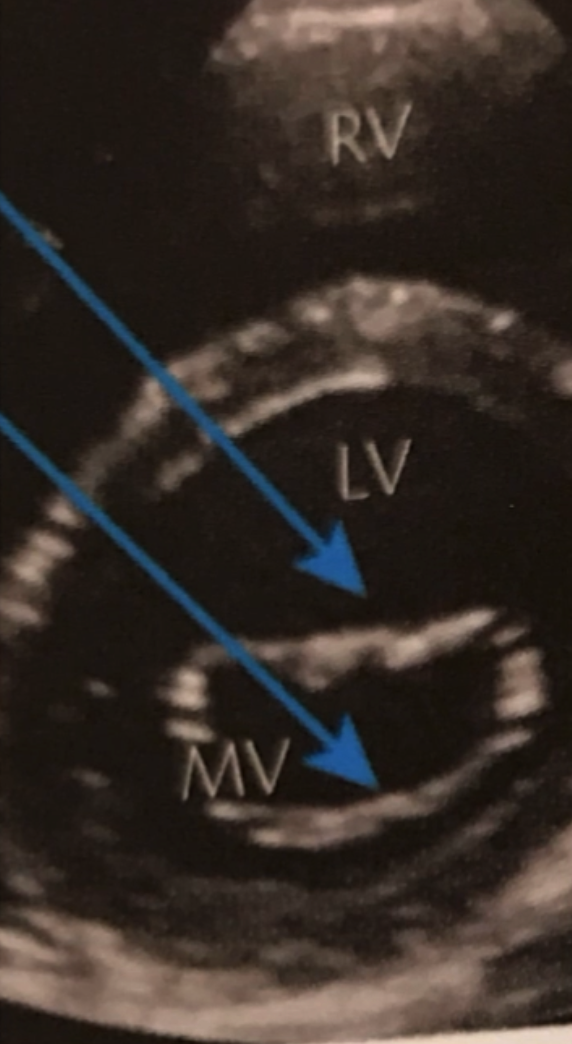
- 在刚才成像的基础上,逐步成角,就可以得到二尖瓣水平的一个成像
- 从上到下可以看到分别是右室、室间隔、左室以及二尖瓣的前叶在上方、后叶在下方

- Tilting the probe tip downward the view of the base of the LV and mitral valve can be seen.
将探头尖端向下倾斜,可以看到左室和二尖瓣底部的视图。 - The ventricle in this view should be round and not oval when done properly.
正确操作时,此切面中的心室应为圆形而不是椭圆形。 - In this view and the next two, many of the 17 different segments of the LV wall can be assessed individually.
在这个切面和接下来的两个切面中,可以单独评估左室壁 17 个不同部分中的大多数。 - Note it is the RV insertion site anteriorly which separates septum from anterior wall and the RV insertion site inferiorly which separates septum from the inferior wall.
请注意,是前部的 RV 插入位点将隔膜与前壁分开,而下部的 RV 插入位点将隔膜与下壁分开。 - Simply assuming the the 12 o’clock position on the LV identifies the anterior wall will not always be correct, especially in hearts that are rotated.
简单地假设左心室上的 12 点钟位置识别前壁并不总是正确的,尤其是在旋转的心脏中。 - AML - anterior mitral leaflet, PML - posterior mitral leaflet
# Papillary Muscle Level
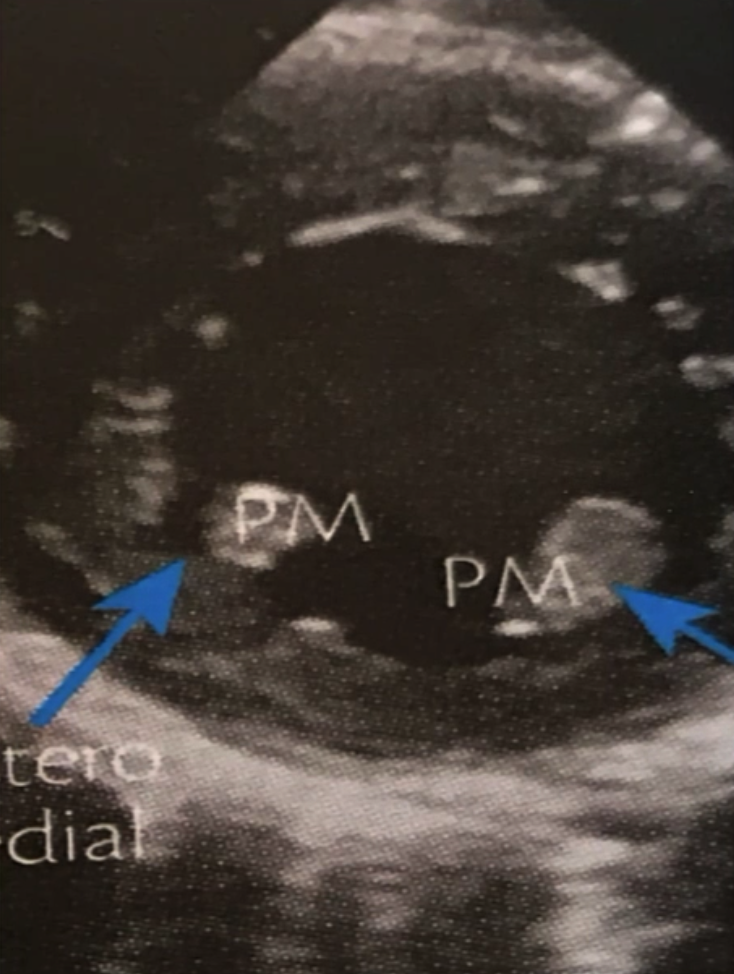
- 探头的方向继续向下倾斜,就可以得到乳头肌水平的成像,大家可以
- 图中蓝色箭头分别指的是乳头肌,以及这个左室中段心肌的成像,可以用来判断左室的收缩功能。

- The mid ventricle level is identified by the presence of the two papillary muscles, which should not be confused for masses or thrombi.
通过两个乳头肌的存在来识别心室中部水平,不应将其与肿块或血栓混淆。 - ALPM - anterolateral papillary muscle. PMPM - posteromedial papillary muscle.
# Apical Level

- 这个声束方向继续向下移动,就可以得到左室心尖的成像
- 如果存在左室心尖部的血栓,在这个图像上也能进行成像。

- Tilting the probe even more inferiorly allows one to see the very apical segment which has no clear papillary muscle structures.
将探头倾斜到更低的位置,可以看到没有清晰乳头肌结构的心室尖。
# The Cardiac Apical Window 心尖声窗

- Assess size and function of the ventricles, atria
评估心室,心房的大小和功能 - Visualisation of the septal and lateral free walls and the apex of the left ventricle
显示室间隔、前侧游离壁以及心尖,和收缩功能的状态 - Mitral and tricuspid valve and the interventricular and interatrial septum seen
可以看到二尖瓣、三尖瓣以及室间隔和房间隔
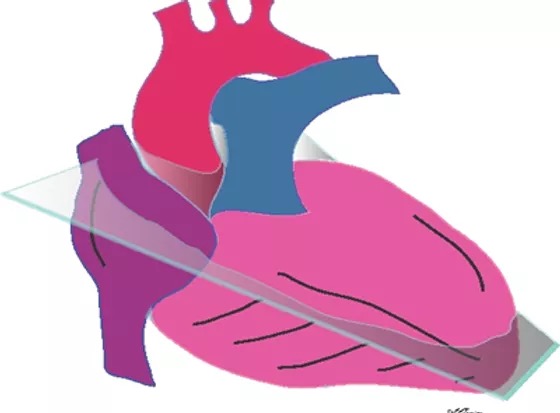
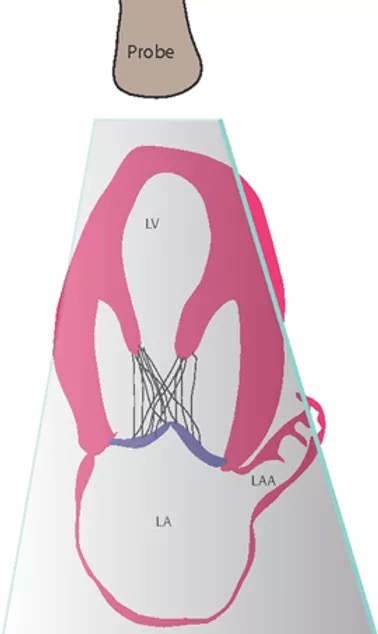
# Apical 4 Chamber view 心尖四腔观

- The apical 4 chamber view is obtained by placing the transducer near the point of maximal impulse with the probe indicator at 3 o'clock.
将探头放置在最大脉冲点附近,探头指示器位于 3 点位置,即可获得心尖 4 腔切面。 - Other apical views will require rotation and tilting.
其他心尖切面需要旋转和倾斜。

- The probe slices through the apex, and right and left ventricles in this view. The atria are in the far field. The field cut of view is such that the aortic root and aortic valve are not seen in this plane.
在这张图中,探头穿过心尖、右心室和左心室。心房在远处。剖切使得在此平面上看不到主动脉根部和主动脉瓣。
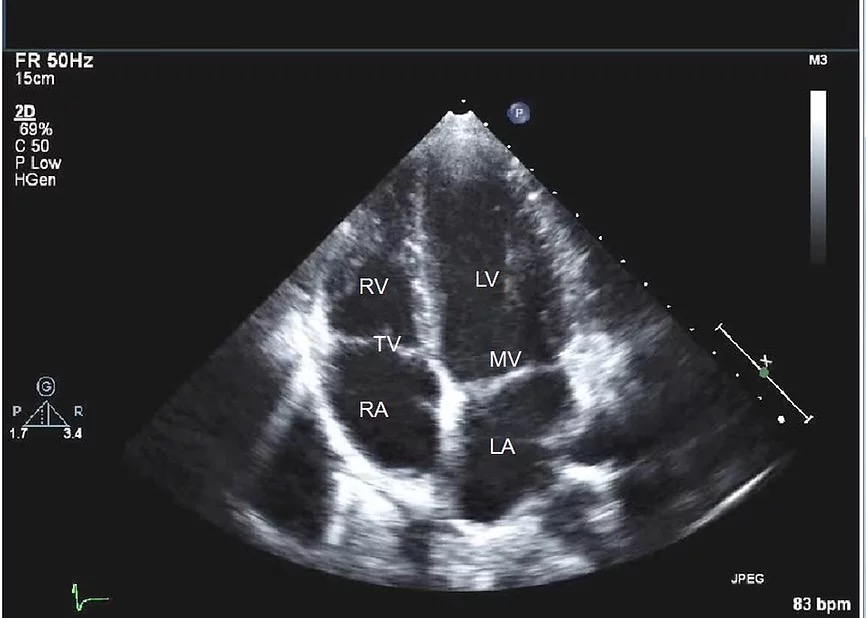
In the appropriate orientation, the septum lines up vertically near the center of the screen.
在适当的方向下,间隔垂直排列在屏幕中心附近。The LV and LV apex should be vertically oriented and the LV should be parabolic in shape as shown.
如图所示,左室和心尖应垂直定向,LV 应为抛物线形状。If the LV apex appears round or is off center you are likely "off axis" which can affect interpretation.
如果 LV 顶点呈圆形或偏离中心,您可能会 “偏离轴线”,这可能会影响解释。该视图还用于评估房车大小和功能、心房大小、心房内和室间隔运动异常以及舒张功能。一些机构将此视图标准化为左右反向,左侧心室位于屏幕左侧,右侧脑室位于屏幕右侧。否则,大多数医院都使用我们上面显示的惯例。LV - 左心室、RV - 右心室、LA - 左心房、RA - 右心房、TV - 三尖瓣和 MV - 二尖瓣。This view is also used to assess RV size and function, atrial size, abnormal intra-atrial and interventricular septal movement, as well as diastolic function.
此切面还用于评估 RV 大小和功能,心房大小,心房内和室间隔运动异常以及舒张功能。A few institutions have standardized this view in right-left reverse with the left ventricle on the left side of the screen and the right ventricle on the right of the screen. The majority of hospitals otherwise use the convention we show above.
一些机构将此切面标准化为左右反向,左侧心室位于屏幕左侧,右侧脑室位于屏幕右侧。其他大多数医院使用上面显示的常规样式。LV - left ventricle, RV - right ventricle, LA - left atrium, RA - right atrium, TV - tricuspid valve, and MV - mitral valve.
In an ideal apical four chamber view, the apex of the left ventricle is at the centre of where the septum and lateral wall meet.
在理想的心尖四腔切面中,心尖位于间隔和侧壁交界的中心;由于心尖四腔心有缺失的问题,可能不能很好的评估是否存在房间隔缺损,所以会运用其他的切面来进行验证。Mitral valve is at a slightly higher position than the tricuspid
valve.
二尖瓣一般比三尖瓣稍高
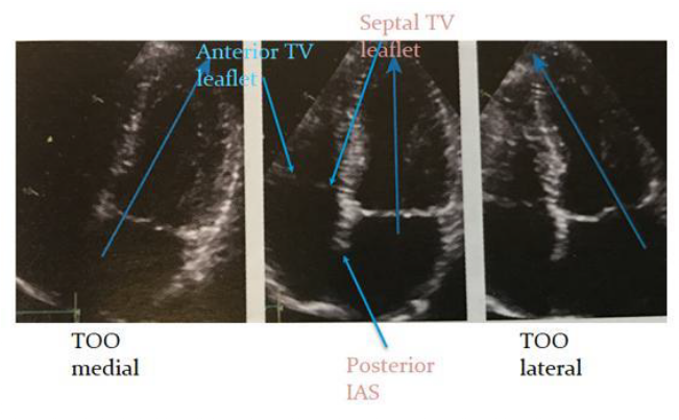
TIPS AND TRICKS
- 获得心尖四腔心的正位图,心尖要正好在探头的下方,像中间的这张图;房间隔室间隔与二尖瓣三尖瓣瓣环呈垂直,二尖瓣三尖瓣瓣环呈水平状。保证测量时的精确度。
- 左侧图显示探头下方是右室,提示探头过于居中、偏右,应该向患者的左侧倾斜。
- 右侧图显示探头下方是心尖,但是靠近侧壁,说明探头偏左,应该向患者右侧偏斜进行调整。
- On axis - The axis is vertical with inter-atrial septum aligned and LV forming the cardiac apex.
轴线上 - 轴线垂直,房间隔对齐,左室形成心尖。- Note tricuspid valve slightly apically displaced compared with mitral (should be < 12mm).
请注意,与二尖瓣相比,三尖瓣略微移位(应小于 12mm)。- Use the LOWEST IC space with a visible view otherwise apex will be foreshortened.
使用视野可见的最低 IC 空间,否则心尖将缩短。- 实际操作中也可以让患者吸气呼气,当观察到最好的心尖四腔心时,让患者屏住呼吸来进行图片抓捕。
- 心尖四腔心的最佳探头位置一般选择最低的一个肋间隙,这样才能保证切的是真正的心尖,而不是这个短切的左室。
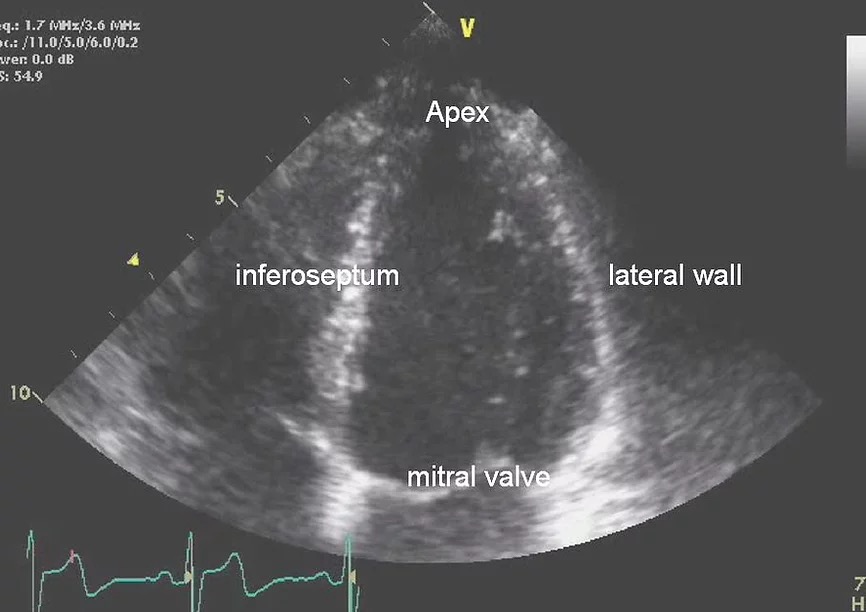
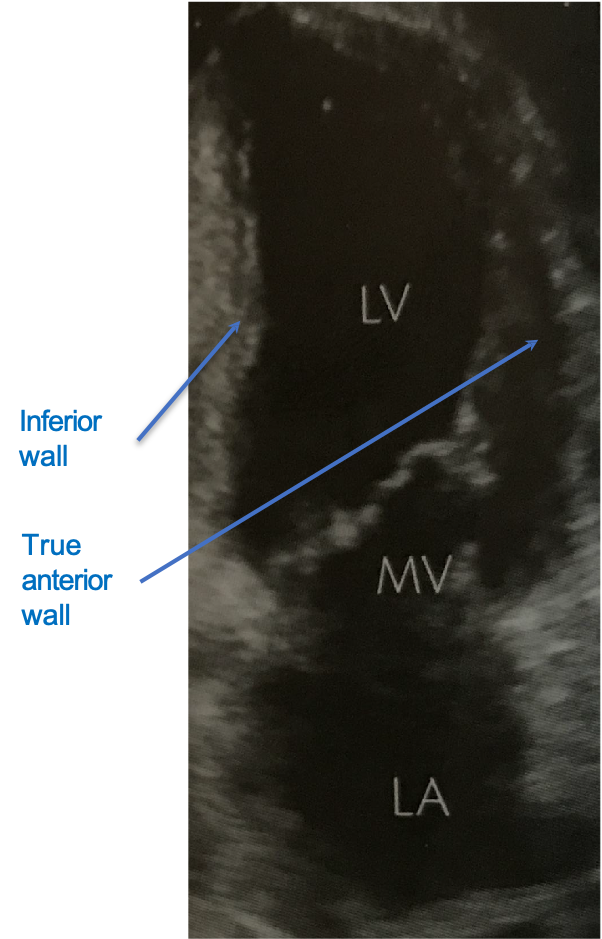
- It is important attempt to get a good look at all of the walls of the left ventricle.
仔细观察左心室的所有壁很重要。 - In this view the inferoseptum, lateral wall and apex can be seen.
在此切面中可以看到间隔、侧壁和心尖。 - The lateral wall is usually the least well seen here because the wall itself is parallel with the ultrasound beam.
在这里侧壁通常是看得最不清楚的,因为侧壁本身与超声束平行。
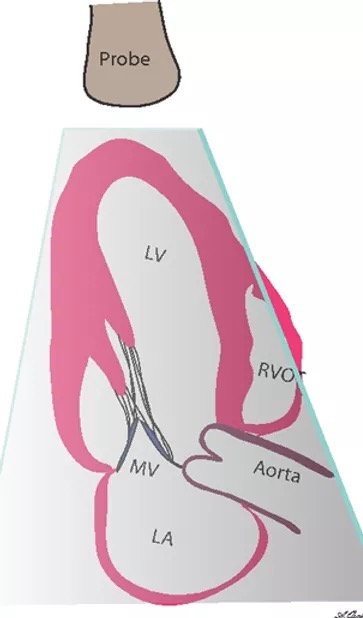
# Apical 5 Chamber view 心尖五腔观

- Tilt probe anteriorly from the 4c position
从 4c 位置向前倾斜探头 - Aortic valve/LVOT(left ventricular outflow tract) comes into view
居中的是主动脉瓣 / 左室流出道,也是主要评估结构 - Anterior part of the IAS(interatrial septum)
房间隔的前部 - LV cavity distorted.
左室腔变形,不能很好的评估左室功能

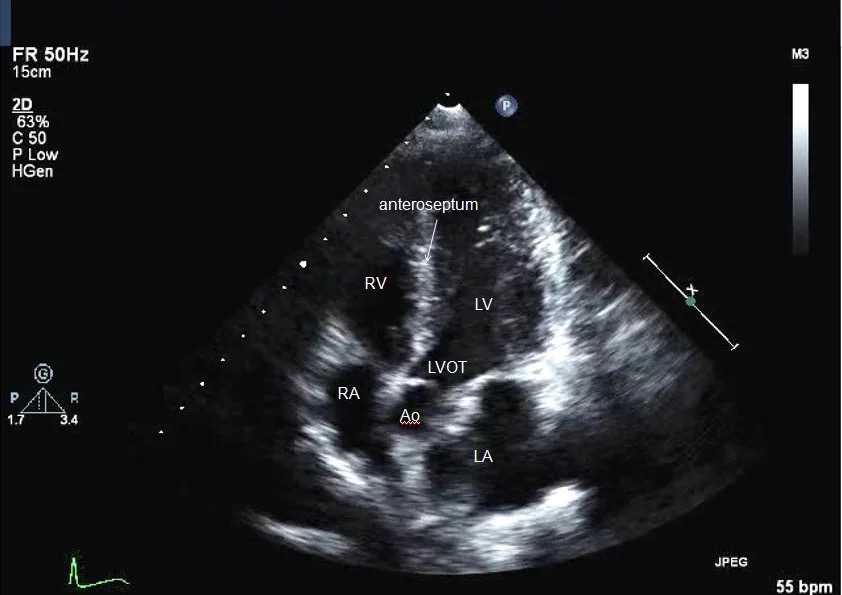
- This is a useful view for evaluating aortic stenosis and regurgitation, and allows Doppler assessment of gradients across the aortic valve in aortic stenosis and measurement of deceleration slopes in aortic regurgitation.
这是评估主动脉狭窄和反流的有用切面,允许多普勒评估主动脉狭窄中主动脉瓣的梯度,并测量主动脉反流中的减速斜率。 - It is also good for the evaluation of the LVOT gradient as seen in cases of hypertrophic cardiomyopathy for example.
也有利于评估 LVOT 梯度,例如在肥厚性心肌病病例中。 - Given that angulation is more anterior, the portion of the septum now visualized in this view is the anteroseptum.
鉴于角度更靠前,现在在该切面中显示的是前中隔。 - Ao - aortic root, RV - right ventricle, LV - left ventricle, RA - right atrium, LA - left atrium.
# Apical 2 Chamber view 心尖两腔观

- Rotation of probe 60° anticlockwise, the apical 2 chamber view can be obtained with the indicator at 12 o'clock.
从心尖四腔心,探头逆时针旋转 60°,指示器在 12 点位置可以获得心尖两腔切面。 - Bi-commissural view of the mitral valve.
二尖瓣双侧交界观
- 上方是左室,下方是左房,居中的是二尖瓣双侧交界。
- 左室的左侧是下壁,右侧是前壁,可以观察左室的收缩功能
- 通过心尖四腔心和两腔心,可以对左室和左房分别进行容积描绘,可以得到左室的射血分数以及左房容积
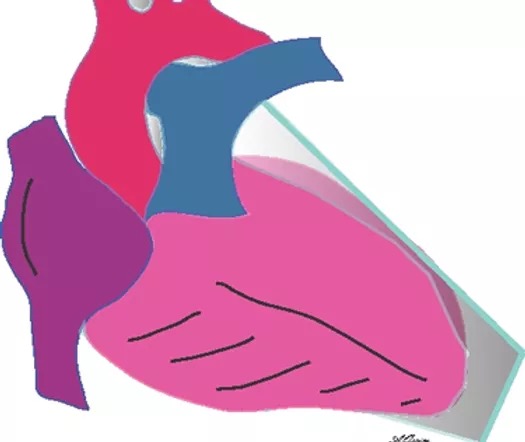
# Apical 3 Chamber view 心尖三腔观

- Rotate anticlockwise further 30°
从心尖两腔继续将探头逆时针旋转 30°,就可以得到心尖三腔 - The apical long axis, sometimes called the three chamber view is obtained by rotation of the probe further counter-clockwise from the apical 2 chamber position to point toward the right shoulder. The probe is thus facing around 10 o'clock (arrow).
心尖长轴(三腔观),是通过将探头从心尖 2 腔位置逆时针旋转,指向右肩而获得的。因此,指示器朝向 10 点钟左右。 - Similar to PTLAX BUT APEX is seen
类似于 PTLAX,但可以看到心尖
wall 后壁;Papillary muscles;Basal and distal lateral septum 基底部和远端外侧间隔")
- 从上到下分别是左室、左房以及右侧的主动脉。
- The anteroseptum now comes into view.
前间隔进入视野。 - Compare this view plane to the parasternal long axis.
将该切面平面与胸骨旁长轴进行比较。 - It is virtually the same except the probe is imaging from the apex.
除了探头从心尖成像外,几乎相同。 - LA - left atrium, MV - mitral valve, LV - left ventricle, RVOT - right ventricular outflow tract.
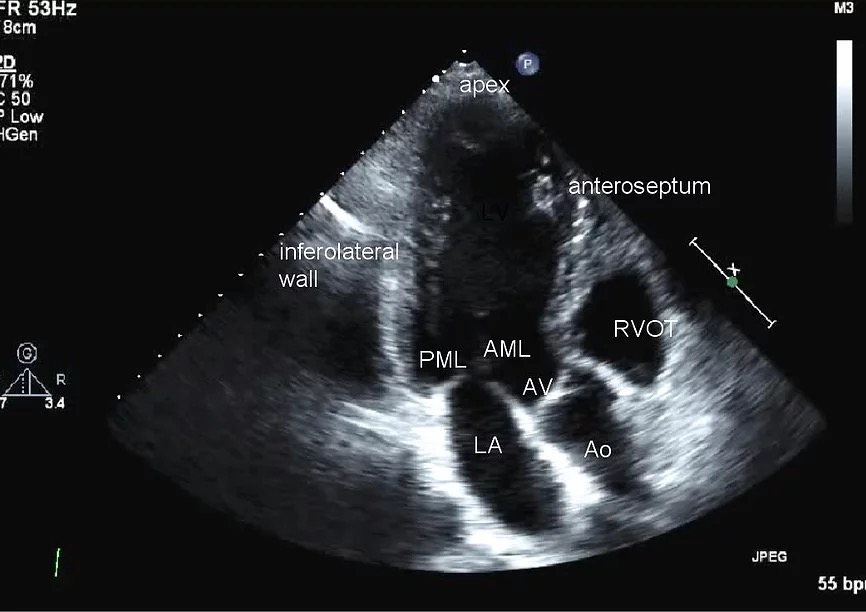
- This view shows similar structures to the parasternal long axis except now the LV apex is well visualized and is in the near field.
- The LV wall segments and views of the aortic and mitral valves are the same.
- Ao - aorta, AV - aortic valve, LA - left atrium, LV - left ventricle, PML - posterior mitral leaflet, AML - anterior mitral leaflet, and RVOT - right ventricular outflow tract.
# Subcostal Views
# Subcostal 4C View

- The patient is placed flat on their back. Sometimes it helps for the head to be slightly elevated or if the patient takes in a deep breath. It may also be helpful if the patient bends their legs.
病人平躺,稍微抬起头或深呼吸、或者弯曲双腿,可能对采集有帮助。 - Scan under the subxyphoid process until a standard 4 chamber view is obtained with the indicator at 3 o'clock.
指示线约在 3 点钟方向 - Increasing the depth is usually needed depending on how high up the heart is located.
根据心脏的高度,通常需要增加深度。


- Probe faces left
探头朝左 - Very clear view of IAS(interatrial septum) and To see a secundum ASD(atrial septal defect)
非常清晰的看到房间隔,并看到第二房间隔缺损 - The heart is now in the far field, and the ultrasound beam has to go through the liver first, before slicing through the right ventricle and then left ventricle.
心脏现在处于远场,超声束必须先穿过肝脏,然后再穿过右心室和左心室。 - The structures seen are roughly similar to the apical four chamber however now the ultrasound beam is more perpendicular to the atrial and ventricular septum.
所见结构大致类似于心尖四腔,但现在超声束更垂直于房间隔和室间隔。 - This view is excellent for looking at the anterior RV free wall, to assess for RV thickness, and for the evaluation of pericardial effusions.
非常适合观察前 RV 游离壁、评估 RV 厚度和评估心包积液。 - It is also one of the most useful views for evaluating flow across the intra-atrial septum for the presence of a PFO or ASD.
对于确定是否存在 PFO 或 ASD,也是评估房内隔分流的最有用的切面之一。
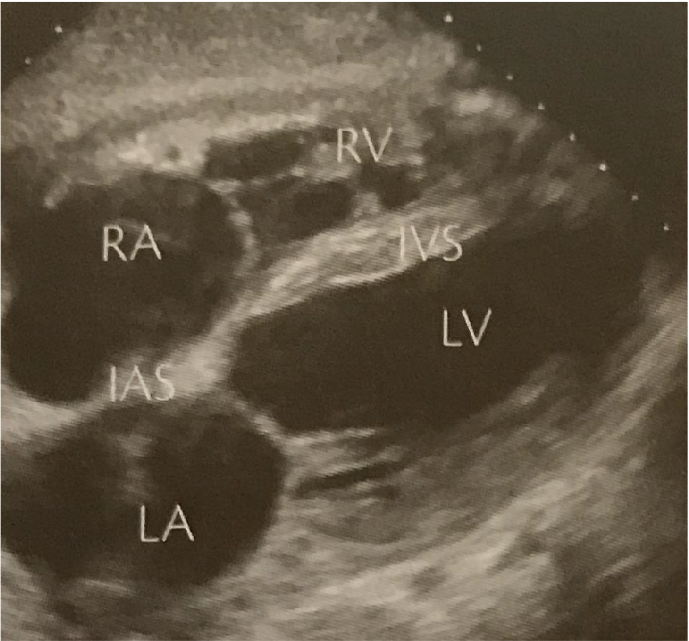
# Subcostal Short Axis
- Rotate probe 90° clockwise form the previous view
从上一切面顺时针旋转探头 90°;指示器大约 1-2 点钟位置。倾斜探头,从心底到心尖逐层扫查。 - This is a similar view to the parasternal short axis of the great arteries
这是与胸骨旁大动脉短轴相似的切面。 - The views here are similar to the parasternal short axis except that we are imaging from a different position. The RV is on the right side in this view.
只是成像角度不同,RV 在右侧。 - If parasternal windows are poor this approach may give more information
如果胸骨旁视窗成像不好,这个切面可能会提供更多信息 - Can measure RVOT(right ventricular outflow tract) diameter and velocities.
可以测量 RVOT 直径和速度。
# IVC views

- probe 90 degrees counter clockwise from the 4 chamber subcostal view so that the probe is pointing toward the head at 12 o'clock.
从肋下 4 腔切面逆时针旋转 90 度,使探头指向头部,在 12 点钟的位置。 - Transducer tilted to RIGHT
传感器向右倾斜 - Tilting medially and laterally will help
show the IVC(inferior vena cava) and aorta
向中间和侧面倾斜会有所帮助,显示下腔静脉和主动脉 - IVC used to estimate RA(right atrium) pressures.
IVC 用于估计 RA 压力

- To get this view, tilt the probe more right lateral from the abdominal aorta view.
要获得此切面,请将探头从腹主动脉切面向右倾斜。 - Alternatively from the subcostal four chamber, visualize the right atrium and turn the probe from the 9 o'clock position to the 12 o'clock position.
或者,从肋下四腔观察右心房,将探头从 9 点钟位置转到 12 点钟位置。 - This view is used to assess RA pressures based on inspiratory collapse of the IVC.
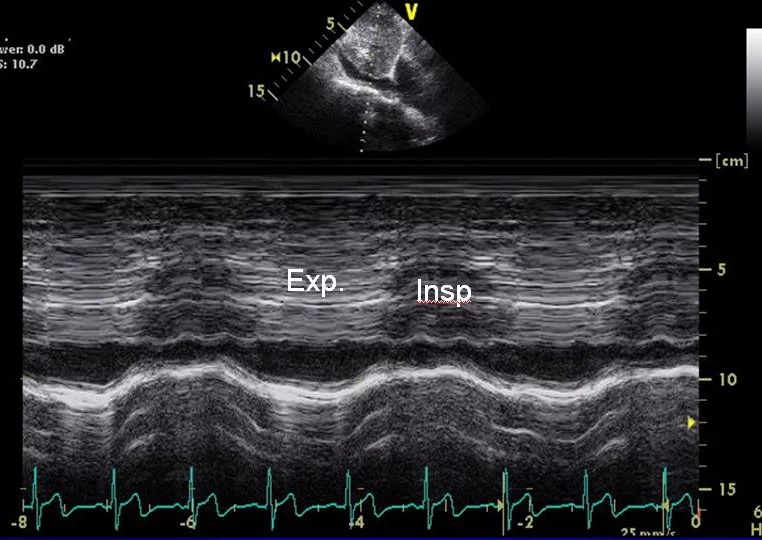
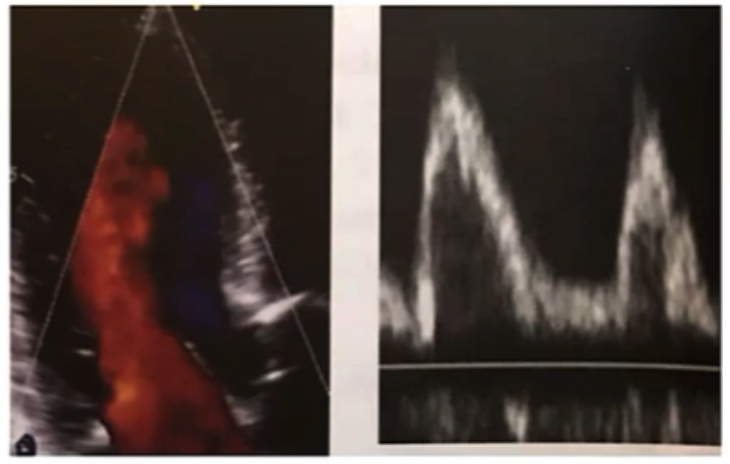
用于根据 IVC 的吸气塌陷评估 RA 压力。 - Lack of collapse suggests high RA pressures where as complete collapse suggests low RA pressures.
无塌陷提示 RA 压力高,而完全塌陷提示 RA 压力低。 - Note the change here in IVC diameter with respiration.
注意下腔静脉直径随呼吸的变化。 - Sometimes an M mode through the IVC as shown above on the right can better help show respiratory changes with time.
通过下腔静脉的 M 模式可以更好地显示呼吸随时间的变化。
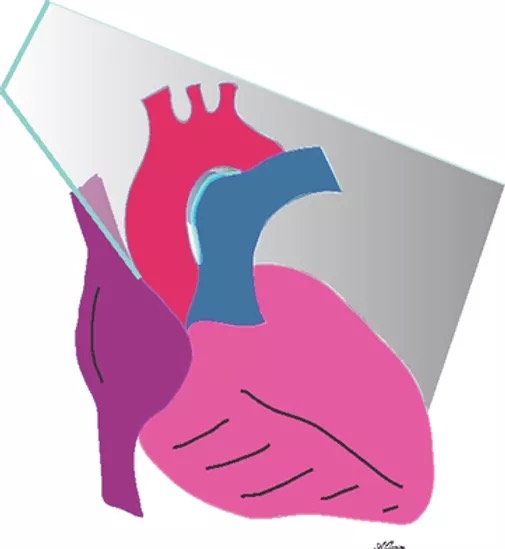
# Supersternal view

Have the patient lie completely flat without anything under the head.
让患者完全平躺,头下无任何东西。Ask them to lift their chin upward and look to the left.
让患者抬起下巴,向左看。Then place the transducer in the suprasternal notch with the probe pointed at the left shoulder at about 2 o'clock.
将探头放入胸骨上切迹,探头指向大约 2 点左右的左肩。Sometimes you may need to tilt the probe to point downward.
有时可能需要倾斜探头以指向下方。胸骨上窝的长轴成像,可以用于主动脉弓部的径线测量,以及降主动脉近端的测量
也可以观察有没有出现主动脉缩窄以及主动脉夹层。
评估重度主动脉瓣反流时,可以放置脉冲多普勒,在降主动脉近端来进行观察有没有反流存在
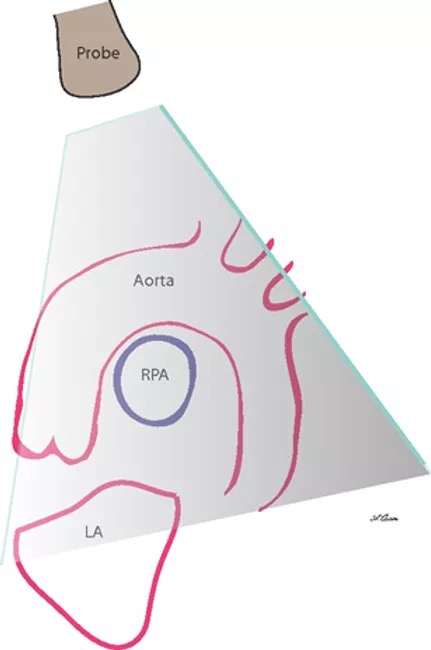
- Note that in this view the right pulmonary artery (arrow) courses underneath the arch, therefore we see it in a short axis view here.
右肺动脉(箭头)位于主动脉弓下方,因此在短轴视图中看到它。 - It is often difficult to see all 3 major branches from the aortic arch. The descending aorta is also less well seen in the far field in this view.
通常很难看到主动脉弓的所有 3 个主要分支。在这张图中,降主动脉在远场也不太清晰。
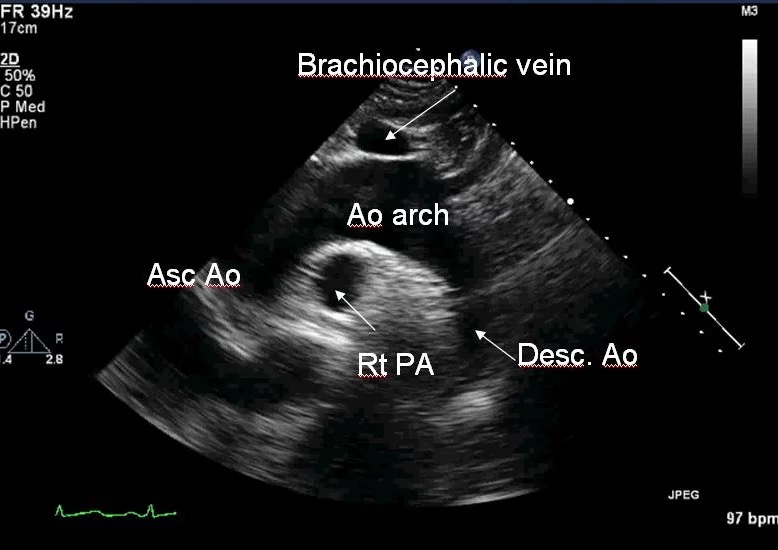
- This view usually gives a nice look at the arch, from which the 3 major vessels may be seen to arise.
这个成像通常可以很好地看到主动脉弓,从主动脉弓可以看到 3 条主要血管。 - The right pulmonary artery and brachiocephalic vein which empties into the SVC can also be seen.
可以看到右肺动脉和头臂静脉流入上腔静脉。 - It is important to use color Doppler to assess flow in the ascending and descending aorta and then to use spectral Doppler.
重要的是使用彩色多普勒来评估升主动脉、降主动脉血流,以及频谱多普勒。
# Doppler Echocardiography 多普勒超声心动图
# Uses
- Valve assessment (will be described in detail in second module) 瓣膜评估
- Valve gradient; valve area; regurgitation volumes
跨瓣压;瓣膜面积;反流容积 - Stroke volume, cardiac output and intra-cardiac shunting
每搏量;心输出量;心内分流 - Estimation of LV filling pressures and diastolic function.
左室充盈压,舒张功能
# Colour Flow Mapping 彩色血流图
- Multiple sample volumes along multiple scan lines
沿多条扫描线的多个取样容积 - Superimposed onto real time 2D image
在实时 2D 图像的基础上叠加 - Colour map used
使用的颜色映射,红色的是流向探头,蓝色的是远离探头 - Visual non-quantitative assessment.
目视非定量评估。也可以进行一些多普勒,像脉冲多普勒、连续多普勒的测量
# Pulsed-wave Doppler PW 脉冲多普勒
- Small and spatially specific sample volume
具有空间特异性 - Low velocities only as misreads flow direction and velocity
仅测量低流速 - Useful to understand spatial presence of a flow.
有助于理解血流的空间位置
# Continuous wave Doppler CW 连续多普勒
- Detects maximal velocity along any given line (the line of the cursor on the 2D image)
检测取样线上最大的血流速度(2D 图像上的取样线) - Low spatial resolution
低空间分辨率 - Detects high velocities.
可以监测到高的血流速度
# How to conduct the examination as a whole 如何进行整体检查
- Complete examination in all patients
对所有患者进行全面检查 - Defined order of acquisition of images and of all Doppler measurements
确定图像和所有多普勒测量的采集顺序 - Measurements can be performed on or offline
测量可以在线上或离线进行 - Report all findings and all structures including normal findings
报告所有检查结果和所有结构,包括正常结果 - Quantitative assessment with significant valve abnormalities
瓣膜明显异常的定量评估 - Sample report and a full examination.
样本报告和全面检查。
# Q&A
左房前后径的测量,在胸骨旁长轴测量和大动脉短轴测量,哪个切面更好,重复性更高?
理论上来讲,从长轴或者大动脉短轴的测量应该都是一样,因为测量的是同一个左房的前后径。但是在实际操作中,要根据这个成像的具体结果,比如有的患者短轴观的左房显示不是很好,这样测量就会存在很大的误差。但是在理论上来讲两个切面的测量是相同的。
因为前后径仅仅是一个二维测量,目前根据最新的指南,建议用心尖四腔 + 心尖二腔进行左房的容积描绘。而且要测量患者的身高体重,算出左房的容积指数,根据容积指数来评估患者的左房是否有扩大的表现。正常的左室形态为圆锥型,当发生形态失常,比如心脏扩大,或者 “S” 形室间隔时,测值误差比较大、重复率低,那这种情况我们应该怎样用二维超声准确评估左室腔大小?
二维超声在 S 形室间隔的测量上确实误差比较大。这种情况下,应尽量避免 M 模式的测量,尽量使用二维测量。其实最好用的是三维测量,或者类似对射血分数的测量,分别在心尖四腔和两腔,对左室进行容积描绘;同时也根据身高体重做出左室使容积指数,能更好地从三维去评估左室是否扩张。
左室的胸骨旁长轴径线测量是一个标准测量,不管患者的室间隔形态是什么,也不论左室是否存在扩张肥厚,都会进行标准测量。系统也会自动在二维测量的基础上,给出射血分数、短轴缩短率等。仅仅是用于参考,还可以运用多种方法来进行综合的评估,这样才能更精确的来评估室间隔的厚度、左室容积,以及左室功能等。