# What is pulmonary hypertension 什么是肺动脉高压
- Elevated pressure in the pulmonary vasculature
肺脉管系统压力升高- Normal mean pulmonary artery pressure is 8-25mmHg.
正常平均肺动脉压为 8-25mmHg。这个参考值是基于右心导管插入术所测得的。 - Pulmonary hypertension is defined by mean PAP > 25mmHg at rest during right heart catheterisation.
右心导管术期间静息时,平均肺动脉压 > 25mmHg 即可定义为肺动脉高压。
- Normal mean pulmonary artery pressure is 8-25mmHg.
| 肺动脉高压程度参考值 | |
|---|---|
| Mild PH | 25 - 40mmHg |
| Moderate PH | 41 - 55mmHg |
| Severe PH | > 55mmHg |
Leads to RV failure due to cor pulmonale.
当肺脉管系统压力升高的时候,右室会做出更大的努力来泵血,最后可能导致右室的衰竭(肺心病)。Symptoms: reduced exercise tolerance, fatigue, syncope, angina, leg oedema, chest pain.
症状:运动耐力降低、疲劳、晕厥、心绞痛、腿部浮肿、胸痛。Right heart catheterisation is the gold standard to confirm the diagnosis of PH and establish the severity.
右心导管术是 PH 确诊和判断严重程度的金标准。TTE can be used to estimate pulmonary pressure.
TTE 可用于(粗略)估测肺动脉压。
因为用超声来评估有很多影响因素,比如当右室收缩功能降低的时候,有可能导致三尖瓣反流的速度过低,则可能低估肺动脉压。
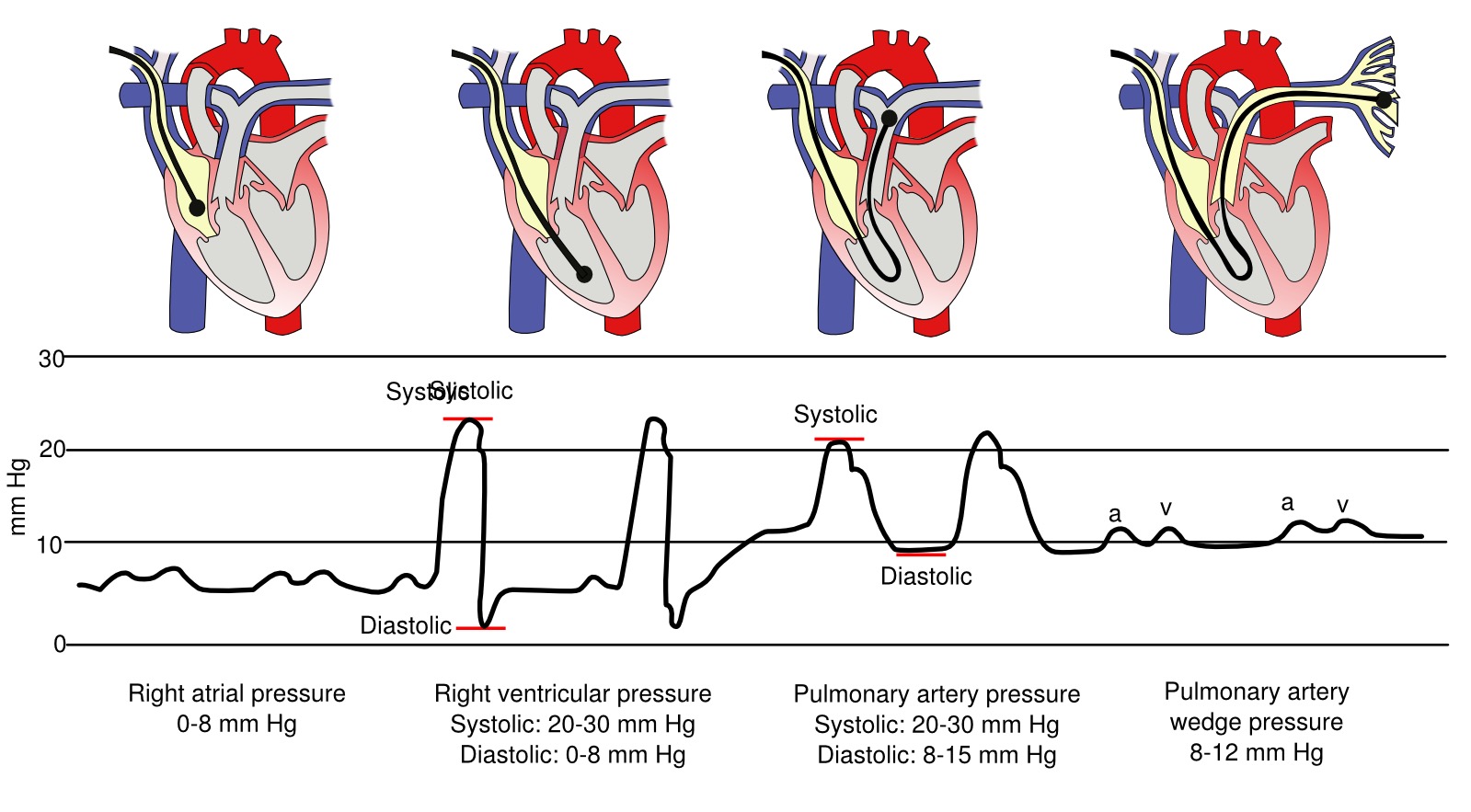
- 将导管从左到右分别放置在右房、右室、肺动脉以及肺毛细血管,以测量不同部位的压力
- 虽然导管放置的位置不同,但是测得的压力基本是一致的;第二和第三张图提示右室收缩压和肺动脉收缩压是基本一致的
- 肺动脉收缩压正常值是 20-30mmHg,舒张压是 8-15mmHg,在定义的时候,用的是肺动脉平均压力(大于 25mmHg)
# Brief classification of PH 肺动脉高压的分类
- Pulmonary artery hypertension (PAH)
原发性肺动脉高压 - PH due to left heart disease
因左心疾病引起的 PH - PH due to Iung disease/ hypoxia
肺病 / 缺氧所致的 PH - Chronic thromboembolic pulmonary hypertension (CTEPH)
慢性血栓栓塞性肺动脉高压 (CTEPH) - PH due to unclear aetiology
不明原因的 PH
# Group 1️⃣ Pulmonary artery hypertension 原发性肺动脉高压
- Diagnosis of exclusion if no other causes found
如果没有发现其他原因而做出的排他性诊断- Idiopathic 先天性的
- Heritable 遗传的
- Drug and toxin exposure 药物和毒素引发的
- Diseases associated with PH 与 PH 相关的疾病
- Connective tissue (scleroderma, SLE)
结缔组织(硬皮病,系统性红斑狼疮 systemic lupus erythematosus) - HIV, portal hypertension
HIV、门静脉高压症 - Congenital heart disease
先天性心脏病
- Connective tissue (scleroderma, SLE)
# Group 2️⃣ Left Heart Disease 左心疾病所致的
- Left ventricular systolic or diastolic dysfunction
左室收缩或舒张功能障碍 - Valve disease.
瓣膜疾病
# Group 3️⃣ Lung Disease 肺病 / 缺氧所致的
- COPD (and less commonly asthma)
慢性阻塞性肺病 / 慢阻肺(少见于哮喘) - Interstitial lung disease
间质性肺病 - Chronic hypoxia
慢性缺氧 - Sleep disordered breathing
睡眠呼吸障碍
# Group 4️⃣ Chronic thromboembolic PH (CTEPH)
慢性血栓栓塞性肺动脉高压
# Group 5️⃣ unclear mechanisms 不明机制的
- Hematologic disorders: chronic haemolytic anaemia, myeloproliferative disorders, splenectomy
血液疾病:慢性溶血性贫血、骨髓增生性疾病、脾切除术 - Systemic: sarcoidosis, pulmonary histiocytosis, lymphangioleiomyomatosis
全身性:结节病、肺组织细胞增多症、淋巴管平滑肌瘤病 - Metabolic disorders: glycogen storage disease, Gaucher disease, thyroid disorders
代谢性疾病:肝糖储积症、戈谢病:影响细胞糖脂类再循环的遗传性代谢病、甲状腺疾病 - Others: tumour obstruction, fibrosing mediastinitis, chronic renal failure on dialysis
其他:肿瘤梗阻、纤维性纵隔炎、透析中的慢性肾功能衰竭
# Assessment of PH 评估
- Estimation of sPAP (or PASP) 肺动脉收缩压
- Other ways to estimate mPAP/dPAP 平均肺动脉压 / 肺动脉舒张压
- Assessment of cardiac cause of PH 原因推断
- Assessment of severity of RV dysfunction 右室功能
- Assessment of prognostic variables 预后因素
# Calculating Right Sided Pressures 计算右侧压力
- RAvol = RVvol = PAvol
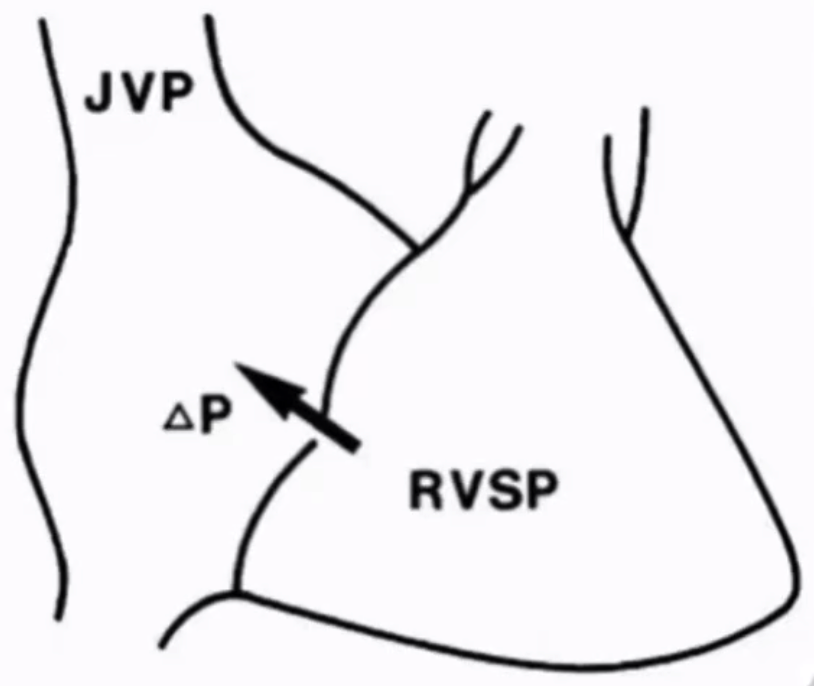
右房容积 = 右室容积 = 右室流出道 / 肺动脉容积 - Pressure gradient between RA and RV is the same as that between PA and RV
RA 和 RV 之间的压力梯度与 PA 和 RV 之间的压力梯度相同,这与前述右室导管测压结果一致 - Hence in the absence of RVOT obstruction:
因此,在没有右室流出道梗阻的情况下:肺动脉收缩压 = 右室收缩压 = 跨三尖瓣压差 + 右房压力
| 肺动脉收缩压 | 参考范围 |
|---|---|
| Normal | < 25 mmHg |
| Mild | 25 to 40 mmHg |
| Moderate | 40 to 70 mmHg |
| Severe | > 70 mmHg |
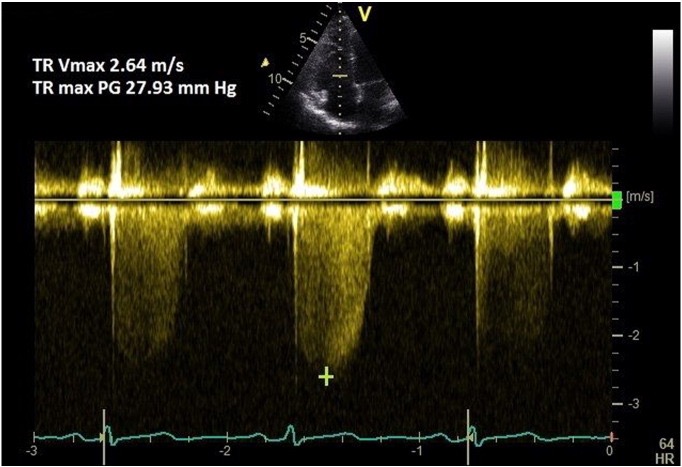
# TR Doppler jet 三尖瓣反流多普勒曲线
Assessed in parasternal RV inflow, parasternal short axis or apical four chamber
在胸骨旁长轴 RV 流入道、胸骨短轴或心尖四腔切面中评估CW 具有一定的角度依赖性,应尽量调节使得取样线和血流平行,这样可以取得最大的反流频谱图。
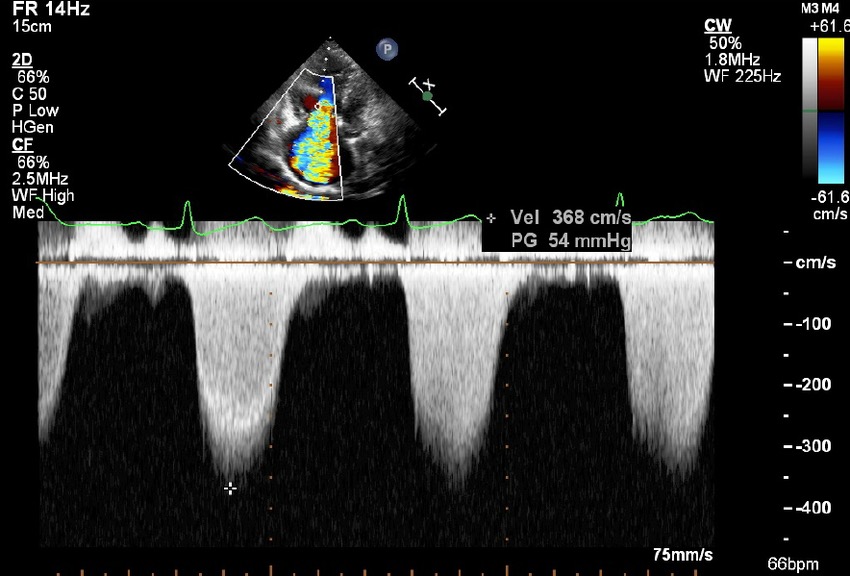
- 右侧频谱图测得了最大血流速度 368cm/s,再通过伯努利方程式,可以得到跨三尖瓣的右室右房压差 54mmHg。
# Bernoulli Equation 伯努利方程
When fluid passes through a narrow space, the velocity increases.
当流体通过一个狭窄的空间时,速度会增加。Pressure is increased before the obstruction and is low behind the obstruction.
压力在阻塞之前增加,而在阻塞之后降低。The difference between these pressures is known as the pressure gradient which can be calculated using the Bernouli equation.
这些压力之间的差值称为压差 / 压力梯度,可以使用伯努利方程计算。简化的伯努利方程式
- In the example above: [1]
which is the pressure change between the RV and RA
简化伯努利方程式在很多运算中都有用到,比如主动脉瓣狭窄进行跨瓣压差测量时。
# Estimate Right Atrial Pressure (RAP) 右房压
- Obtain the IVC in subcostal window
剑突下切面得到 IVC 成像 - Ask the patient to sniff - mimics inspiration - and assess collapsibility of the IVC.
让病人快速吸气 - 模仿吸气,并评估下腔静脉的崩溃 / 塌陷
- 建议在靠近右房大概 1cm 左右,约在肝静脉(hepatic vein)水平进行采样
| 1️⃣ Size of IVC | 2️⃣ IVC size On Inspiration | Right atrial pressure(mmHg) |
|---|---|---|
| Small < 1.5cm | Near total collapse | 0 - 5 |
| Normal(1.5-2.5cm) | Decrease > 50% | 5 - 10 |
| Normal | Decrease < 50% | 10 - 15 |
| Dilated > 2.5cms | Decrease ≤ 50% | 15 - 20 |
| Both IVC & Hepatic veins dilated | No change | > 20 |
# Echocardiographic images of methods for estimating mPAP
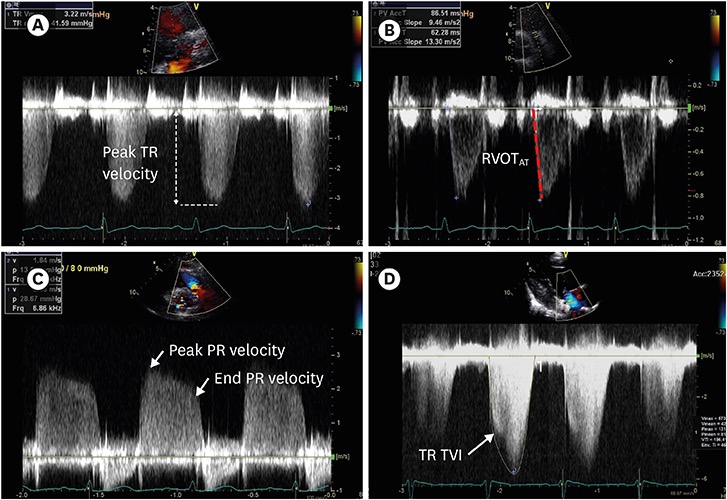
- Estimation of mPAP using peak TR velocity (A); RVOTAT (B); peak and end PR velocity (C); and TR velocity TVI (D). mPAP: mean pulmonary artery pressure, PR: pulmonary regurgitation, RVOTAT: right ventricular outflow tract acceleration time, TR: tricuspid regurgitation, TVI: time velocity integral. [2]
# mPAP from PASP 通过肺动脉收缩压计算平均肺动脉压
- Mean pulmonary artery pressure (mPAP) can be estimated from PASP
平均肺动脉压可以通过肺动脉收缩压估计 - mPAP is the measurement used during right heart catheterisation.
mPAP 是右心导管插入术期间使用的测量值。
- Therefore a PASP of 40mmHg is equal to mean PAP of 25mmHg
因此,40mmHg 的 PASP 等于 25mmHg 的 mPAP - Can also calculate the mPAP using pulmonary flow dopplers.
也可以使用肺血流多谱勒计算 mPAP
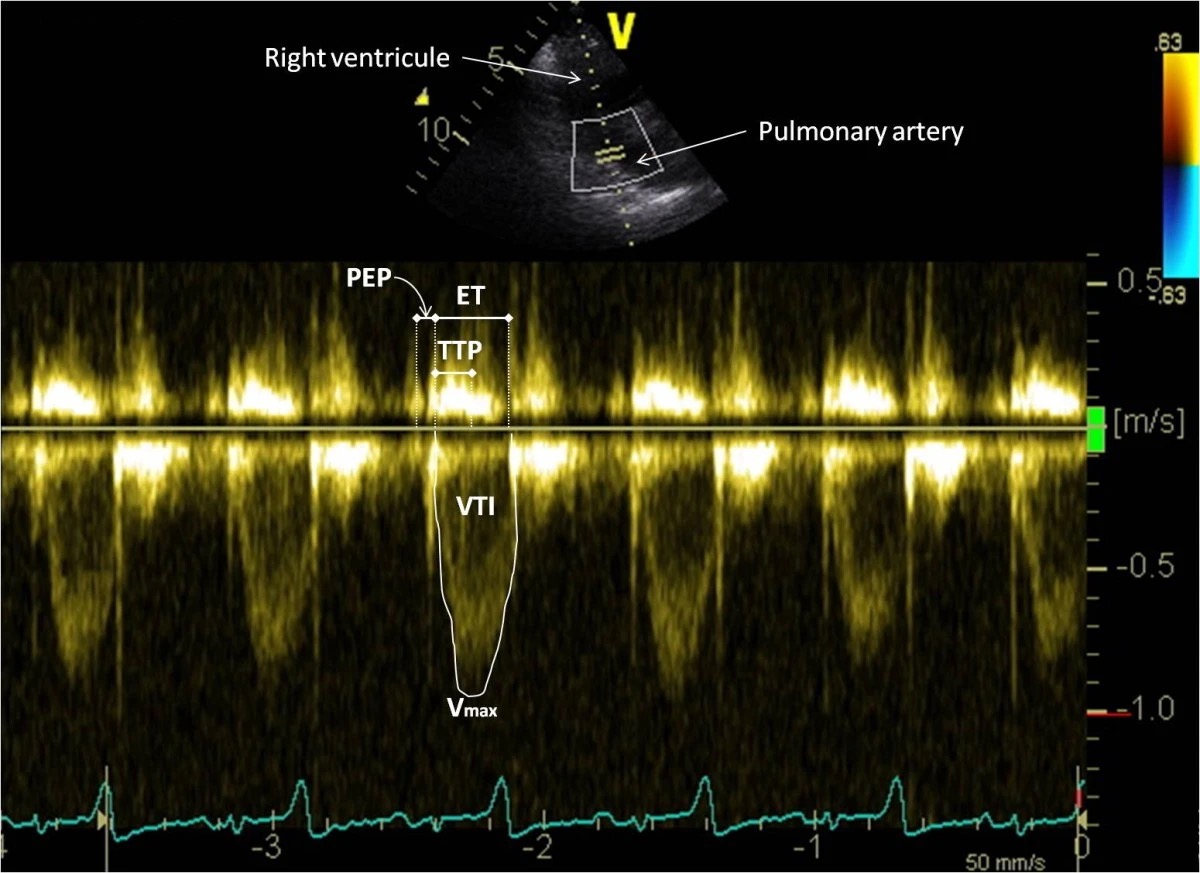
# mPAP from PV Acceleration Time 肺动脉瓣加速时间计算平均肺动脉压
- Assessed using PW doppler in the PSAX window at the RV outflow
在右室流出道的 PSAX 切面中使用 PW 多普勒进行评估

 focus on AV")
 focus on PV")

Note the monophasic shape of the Doppler waveforms.
注意多普勒波形的单相形状。Measurements of peak systolic velocity (PV-Vmax), acceleration time (PV-Acc Time), and velocity–time integral (VTI) are shown on the Doppler spectrum. PV, pulmonary valve.
多普勒频谱上显示了收缩期峰值速度(PV Vmax)、加速时间(PV Acc 时间 = 44ms,从肺动脉瓣基线状态开始打开到达峰值即最大流速度的时间,通过公式可以计算得到 mPAP 平均肺动脉压)和速度 - 时间积分(VTI)的测量值。PV,肺动脉瓣。For example in the case shown here:
# PV Acceleration Time 肺动脉瓣加速时间
- Can use the PV acceleration time in isolation to estimate pulmonary pressures
可以单独使用 PV 加速时间来估计肺动脉压
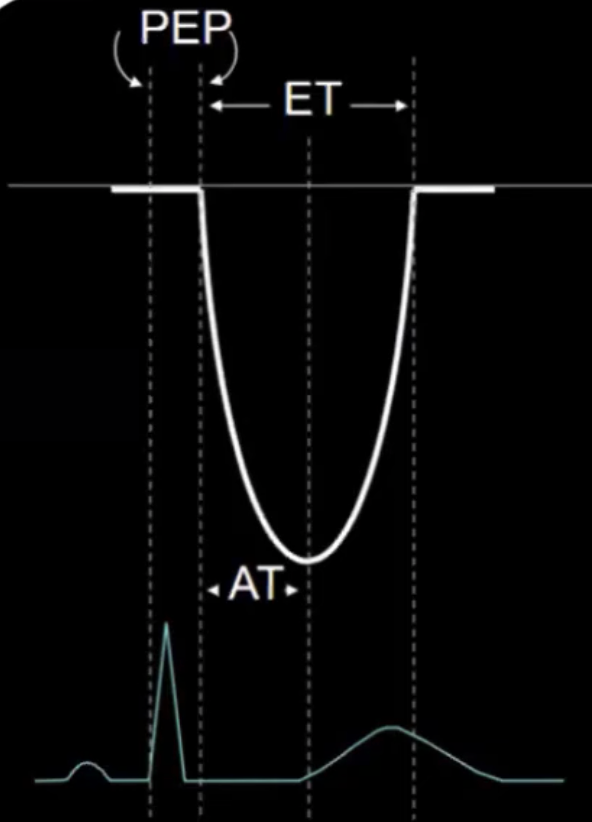
- Pulmonary outflow velocity spectrum obtained from a right parasternal right ventricular inflow-outflow view.
从右胸骨旁右室流入 - 流出切面获得的肺流出速度频谱。 - The peak velocity of the pulmonary flow (Vmax), the velocity time integral (VTI), the ejection time (ET), the time to peak velocity (TTP) and the pre-ejection period (PEP) of the pulmonary flow were measured as shown.
测量肺血流峰值速度(Vmax)、速度 - 时间积分(VTI)、射血时间(ET)、峰值速度时间(TTP)和射血前时间(PEP),如图所示。
| PV Acceleration Time | |
|---|---|
| Normal | > 130ms |
| Borderline 临界 | 100 - 130ms |
| Confirmed | 80 - 100ms |
| Severe | < 80ms |
一般临床怀疑有肺动脉高压时才测加速时间,一般不常规测
# dPAP or mPAP from PR Jet 肺动脉瓣反流曲线计算肺动脉舒张压或平均肺动脉压
Assessed using continuous wave doppler in the PSAX window at the RV outflow
在右心室流出道的 PSAX 切面中使用连续波多普勒进行评估Line up with the PR jet
在肺动脉瓣反流束放置采样线


分别通过伯努利方程式计算
PR end diastolic pressure gradient, 肺动脉瓣反流舒张末期压力梯度
PR peak pressure gradien, 肺动脉瓣反流峰值压力梯度
# Assessing the Right Ventricle in PH
Acute Pulmonary Hypertension 急性肺动脉高压
- Due to sudden increase in pulmonary vascular resistance e.g. acute severe MR, massive pulmonary embolism
由于肺血管阻力突然增加,例如急性重度二尖瓣反流、大范围肺栓塞 - Right ventricle dilates first
右心室先扩张
- Due to sudden increase in pulmonary vascular resistance e.g. acute severe MR, massive pulmonary embolism
Chronic Pulmonary Hypertension 慢性肺动脉高压
- Pressure overload: RV hypertrophy and then dilatation
压力负荷过高:右心室肥厚,然后扩张;栓塞或肺动脉瓣狭窄引起 - Volume overload: RV dilatation.
容量负荷过高:右室扩张;三尖瓣反流或肺动脉瓣反流所致
- Pressure overload: RV hypertrophy and then dilatation
# Assessing Right Ventricular size in PH
# RV inflow Dimensions

| Assessed in apical 4 chamber | 右心室内径 | |
|---|---|---|
| Base (RVD1) | below the TV annulus 基底部 | < 4.2cm |
| Mid (RVD2) | mid-RV cavity at level of MV papillary muscles 中部 | < 3.5cm |
| Length (RVD3) | base to apex 到心尖的长径 | ≤ 8.6cm |
# RV Outflow Dimensions
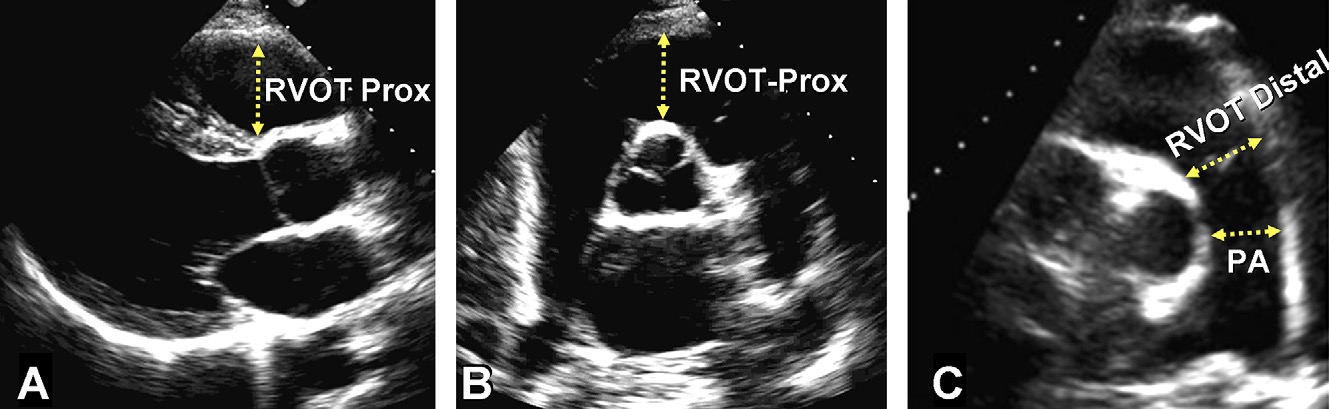
| Parasternal long axis | ||
|---|---|---|
| RVOT Prox in PLAX | 近端内径 | < 3.1cm |
| RV:LV cutoff ratio | > 0.5:1 in PH | |
| Parasternal short axis | ||
|---|---|---|
| RVOT Prox at AV level | 近端内径 | < 3.6cm |
| RVOT distal at PV level | 远端内径 | < 2.8cm |
| PA diameter | 肺动脉内径 | < 2.3cm |
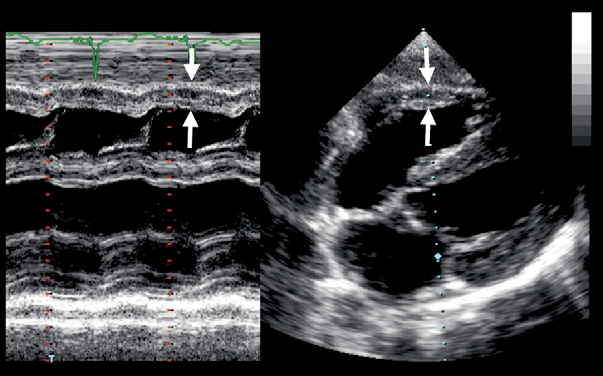
# RV Wall Thickness
慢性肺动脉高压中
- Assessed in subcostal or parasternal long axis
在剑突下或胸骨旁长轴切面评估 - > 5mm represents RVH which is seen most commonly in pressure overload conditions
表示在压力过载情况下最常见的 RVH - Measure at the level of TV chordae at R wave.
在 R 波(舒张末期)的 TV 腱索水平上测量
. LA left atrium, RA right atrium, LV left ventricle, RV right ventricle 剑突下四腔心中显示的RV壁厚增加 (白色箭头)。LA左心房、RA右心房、LV左心室、RV右心室")
# Assessing RV dysfunction 右心功能的评估
# TAPSE (Tricuspid Annular Plane Systolic Excursion) 三尖瓣环平面收缩期偏移
- Apical 4 chamber window
心尖四腔心
存在角度依赖性,因为要切到较为正位的心尖四腔切面,没有任何不准确的伪像,间隔和腔室看起来尽可能垂直 - Degree of systolic excursion of the tricuspid annulus
三尖瓣环收缩期偏移程度,评估右室纵向收缩功能
| TAPSE | |
|---|---|
| Normal | ≥ 16mm |
| Mild | 13- 15mm |
| Moderate | 10-12mm |
| Severe | <10mm |
- Reproducible technique.
可重复使用的技术 - 当右室存在明显扩张时,可能很难得到标准的心尖四腔心切面,此时应尽量的使取样线和三尖瓣瓣环呈现垂直的状态
# Other Techniques to Assess RV Function in Pulmonary Hypertension
Apical 4 chamber window
心尖四腔心Pulsed wave doppler (with TDI) in the middle of the basal segment of the RV free wall
右室游离壁基底段中部的脉冲波多普勒 (带 TDI)S' is the highest systolic velocity
S’是最高收缩期速度Impaired RV if S’ < 12cm/s.
当 S’<12 cm/s 时,RV 受损。Can also calculate MPI with TDI: impaired RV function if ≥ 0.55
也可以用 TDI 计算 MPI 心肌做功指数:如果≥0.55,RV 功能受损
# Pressure Overload 压力负荷过高
- Septum flattens in systole and diastole
室间隔在收缩期和舒张期变扁平 - the eccentricity index can quantify this.
可用偏心指数量化 - Causes 原因
- Pulmonary hypertension 肺动脉高压
- Acute pulmonary embolism 急性肺栓塞
- RV outflow tract obstruction 右室流出道梗阻
# RV Dilatation - Volume Overload 容量负荷过高
Atrial septal defect, partial anomalous pulmonary venous drainage, coronary sinus defect
房间隔缺损、部分型肺静脉异位回流、冠状静脉窦型缺损Tricuspid valve disease 三尖瓣疾病
Ebstein anomaly 畸形
Pulmonary regurgitation 肺动脉瓣反流
RV outflow tract obstruction 右室流出道梗阻
The septum flattens during diastole
舒张期室间隔变扁平the eccentricity index can quantify this.
可用偏心指数量化
# Eccentricity Index (EI) 偏心指数
D1 = Minor axis dimension perpendicular to septum
垂直于室间隔的短轴尺寸D2 = Minor axis dimension perpendicular to D1
垂直于 D1 的短轴尺寸EI cutoff > 1.0
- If EI > 1 in systole it suggests a pressure overload state
发生在收缩期时,表示压力超负荷状态 - If EI > 1 in diastole it suggests a volume overload state
发生在舒张期时,表示容量超负荷状态
- If EI > 1 in systole it suggests a pressure overload state
# Prognostic features on echo 超声下的预后特征
# Prognostic Indicators 预后指标
- There presence of the following on echocardiography suggest a worse prognosis in patients with PH:
超声心动图上存在以下情况表明 PH 患者的预后较差:- Right atrial dilatation
右房扩张 - Chronic pericardial effusion
慢性心包积液 - RV dysfunction
右室功能障碍 - LV compression due to RV dilatation
右室扩张引起的左室压缩 - Reversal of septal curvature with slit like LV
室间隔曲度反转伴狭缝样左室 - Tei index of RV (myocardial performance index).
右室 Tei 指数 (心肌功能指数)
- Right atrial dilatation
# Suggested PH Studly
- If PH is suspected e.g. if
如果怀疑有肺动脉高压,例如发现- TR Vmax >2.6m/s
三尖瓣反流最大速度 > 2.6m/s - dilated RV
右室扩张 - TAPSE < 1.6cm
- dilated IVC
下腔静脉扩张 - dilated RA
右房扩张
- TR Vmax >2.6m/s
- Perform right heart protocol:
应进行右心检查- RV Tei index
右室 Tei 指数 - TDI RV free wall
TDI 右室游离壁 - eccentricity index
偏心指数
- RV Tei index
- Assess associated causes:
评估相关原因:- Look for ASD / VSD / PFO
检查房间隔缺损 / 室间隔缺损 / 卵圆孔未闭 - Moderate to severe mitral valve disease
中至重度二尖瓣病变 - LV systolic impairment
左室收缩功能受损 - LV diastolic impairment
左室舒张功能减退
- Look for ASD / VSD / PFO
# Q&A
超声评估肺动脉平均压与有创评估的肺动脉平均压相关性如何?
右心导管检查是金标准,超声只是一个粗略评估的手段。
有很多的影响因素会使得超声评估肺动脉收缩压,不太精确性,比如有角度依赖性,以及当右室功能受损的时候,测量值会受到影响。
右心导管是侵入性检查,有并发症风险,因此我们应该先做超声心动图筛查有无肺动脉高压。
如果超声完全正常,则基本不会有肺动脉高压;如果超声不正常,则提示可能存在肺动脉高压,如果同时也有症状,则可以考虑做右心导管检查确诊。房颤患者的右心房压力评估方法也是一样的吗?
当存在房颤时,仍然可以根据腔静脉回缩率,来进行右房压的评估。但是可能需要取多个心动周期来进行平均值的计算,一般至少需要取三个以上的心动周期,来测量尺寸以及回缩率的情况。
因为,目前 ESC 和 BSE 对肺动脉压的评估都是用进行可能性评估,需要结合 TR 测量及一些间接指标,那么应用肺动脉瓣测量平均压是否更为直接或者准确?因为有些扩心病或者缺血性心脏病患者有时测不到明显的 TR。
对于肺动脉高压,右心导管插入术仍然是金标准,超声心动图只是对肺动脉收缩压进行一个可能性的评估。在超声中,其实是把几个方法融合到了一起,比如需要根据 TR 来测量一些指标,同时加速时间是在肺动脉瓣进行测量的,也就是说超声把多种方法融合到了一起,来进行综合的可能性评估,看有没有肺动脉高压。
超声心动图中每种方法都有各自的缺陷,比如有的患者测不到 TR,有的患者在不同次测量时,如果心率存在不同,那么对肺动脉瓣的加速时间也是有明显影响的。超声心动图的方法,没有一个是能很准确的来进行测量的,仅仅是靠多种方法进行一个综合性的一个分析判断。